COGNITIVE BEHAVIORAL THERAPY FOR
PSYCHOSIS HANDOUTS
Valerie Kreider, Ph.D., LPCC-S, LICDC-CS
Harry Sivec, Ph.D.

1
Contents
Getting to Know your Client 3
Time Line…………………………………………………………………….….…… 4
Personal Goal Setting……………………………………………………..…… 6
Formulation 9
Formulation for Case Management………………………..……….….. 10
Making Sense Formulation (for Licensed Practitioners)…….… 12
Engagement Strategies 13
Engagement Strategy Check Sheet……………………………… .….…… 14
Clinical and Adaptive Mode Comparison………………………..…….… 15
What is Psychosis……………………………………………………….…..…...… 17
Working with Thoughts and Cognition 22
Aspects of Experience……………………………………………….…….…….. 23
Common Unhelpful Thinking Styles…………………………….….……… 24
What do We Know about Thoughts………………………….….………… 26
The Three Step Technique………………………………………….….………. 27
Practicing the Three Step Technique……………………………..….…… 31
Alternative Explanations………………………………………………………… 32
Working with Thoughts Practice…………………………..………..……... 34
Changing Troubling Thoughts………………………………………….…….. 35
De-centering…………………………………………………………….…….……... 36
Thought Record for Belief (and blank worksheets)………...….….. 37
360⁰ Pros and Cons (and blank copy)..……………………………….….. 41
Working with Emotions 43
Emotion Chart…………………………………………………….……….….…….. 44
Mood Diary……………………………………………………………………………. 45
Mindfulness Techniques
Grounding………………………………………………………….……… 46
Relaxation………………………………………………………….……… 47
Breathing………………………………………..………………….…….. 48
Mindfulness and Working with Voices………………….…… 49
Mindfulness Practice and Survey…………………………….… 50
Emotion Regulation and the Brain……………..…………………….……. 52
The Stress Bucket………………………………………………………..….…….. 54
Working with Behaviors 61
Behavioral Experiment……………………………………………………………. 62
Setting up the Investigation……………………………………………….……. 63
The Investigative Analysis Worksheet .……………………….…………… 64
Investigation Analysis Worksheet with Demo………….………………. 65
Blank Worksheets……………………………………………………………………. 66
Working with Voices and Hallucinations 68
Voice Diary…………………………………………………………….……………….. 69

2
Some Ideas about How to Cope with Voices…………….…..………… 70
Coping with Voices or Experiences………………………………..………… 87
List of Coping Strategies for Hallucinations……………...……………… 88
Working with Negative Symptoms 90
Daily Schedule……………………………………………………………………….… 91
Negative Symptoms…………………………………………………………………. 92
Positive Symptoms…………………………………………………………………… 93
Working with Delusions 94
Delusions Level 1 & 2………………………………………………………………… 95
CBTp Methods for Working with Delusions………………………………. 96
Special Topics 98
Suicide…………………………………………………………………………………….… 99
Homicide………………………………………………………………………….…….…. 100
Crisis Planning………………………………………………………………….………… 101
Adherence____________________________________________ _ 102
Adherence Factors……………………………………………………………………. 103
Adherence Solutions Card………………………………………………….……… 105
My Values and Goals…………………………………………………………………. 106
Outcome Measures 107
Beliefs about Voices Questionnaire (BAVQ)……………….……………… 108
Psychosis Symptom Rating Scale (PSYRATS)………………………………. 110
Recovery Assessment Scale: Domains and Stages (RAS-DS)…..…… 113
DIALOG……………………………………………..….……………..……………………. 116
Study Guides 118
Section 1.1: Introduction……………..……………………………………………. 119
Session 1.2………………………………………………………………………………... 120
Session 1.3………………………..………………………………………………………. 122
Session 2.1………………………………………………………………………..………. 124
Session 2.2………………………………………………………………………………… 126
Session 2.3………………………………………………………………………………… 128
Session 2.4……………………………………………………..…………………………. 130
Session 3.1………………………………………………………………………………… 132
Session 3.2……………………………………………………………………..…………. 134
Practicum Instructions 135
3
Getting to Know Your Client

4
Timeline
Age/Year
Experience
Health, Family, Education/Job, Significant Life Events, etc.
Meaning
What it meant to me at the time (e.g. I
was alone, unloved, unfairly treated,
others hurt me, rejected me…)
0 to 5
6 to 10
11 to 15
16 to 20
5
Timeline
Age/Year
Experience
Health, Family, Education/Job, Significant Life Events, etc.
Meaning
What it meant to me at the time (e.g. I
was alone, unloved, unfairly treated,
others hurt me, rejected me…)

6
Personal Goal Setting
1. Working from Values: It is helpful to develop personal goals from some value(s) that
we hold dear to our heart (such as family, worship and faith, work, friendship). Values
help us to know what is important in our life to feel really good about ourselves.
2. Identify some of your strengths – the things that you are (or were) good at, felt good
about, celebrated within yourself, that can become a goal or can help you reach your
goals. Maybe volunteer at an animal shelter, find a used instrument to play, experiment
with things you loved to do, but find yourself shying away from now.
3. Personal Goals: These are goals that people want to reach in order to better their own
lives. Reaching personal goals can create a sense of self-empowerment and success.
They can help to guide us back to what we are working for in our life.
Sample Values:
• Faith/Spirituality
• Family
• Independence
• Humor
• Adventurousness
• Compassion
•
Friendship
•
Honesty
•
Gratitude
• Responsibility
• Believing in yourself
•
Courage
•
Success
•
Creativity/Art
• Animal Lover
Sample Strengths:
• Good with people • Willing to ask for support
• Good with animals • Follow through on tasks
• Play the guitar/piano/instrument • Responsible
• Motivated • Hard worker
Sample Goals:
• Solving an ongoing problem
• Making it to appointments on time
• Re-connecting with the people with in your life relationships
• Taking better care of your health (eating well, losing weight, quitting a habit)
• Have some fun in your life
• Begin dating again

7
4. Decide on one or two goals to start with: It’s really hard to work on more than a couple
goals at a time. Start with one thing you would like to work towards right now. The
process of setting goals helps us to stay on track in our everyday life. If we can take care
of our goals each day, we are much more likely to reach a bigger goal down the line.
5. Define “Stepping Stones”: Creating a set of small goals can help us to achieve a large
and important goal. For example, if we want to get across a river, there may be several
steps involved before actually being able to cross it (finding a boat, finding supplies to
build a bridge, confronting a fear of water, etc.). So Stepping Stones are the small goals
we set that will lead us to reaching the bigger goal.
6. Review the goal you have set for yourself along the way:
1. What kind of progress have you made (0% to 100%)
2. What has gotten in your way of working toward the goal?
a. Unexpected obstacles along the way
b. Goal was too big
c. Discovered that the goal is no longer attractive
d. Keep forgetting the goal on a day to day basis
e. There may be many more valid reasons why someone might not hit the goal
target……
3. What kind of problem solving might help reach the goal, to overcome the barriers?
7. Rework the goal until you find it doable for you and on a time line that is right for you:
There is nothing wrong with continuing to work on a goal in the way you have been,
modifying it so that it is easier to keep track of and accomplish, or throwing the goal out
and starting with a new one. It’s your life, and so they are your goals. We are here to
support you in any way we can to help you reach the goals you want to reach.
Let’s say the goal is to “make it to my 3 appointments on time in the month of May
Sample Stepping Stones:
• Acquire a calendar (paper calendar, or use a calendar app on your phone)
• Write in your appointments on the calendar
• Set an alarm for yourself
• Keep all of your appointment reminder cards in one place
• Ask someone to remind you (ask if you can have a reminder call)
• Practice reviewing your calendar daily for 10 minutes

8
Goal # Recovery Enhancement Plan
Brainstorming…..What area of your life would you like to improve?
Values:
Strengths:
What obstacles might you face in trying to reach your goal?
Decide on Long Term Goal:
Target Date:
Stepping Stones and Target Dates: Target Date:
If the plan isn’t working as you wanted it to, there are three options (circle one):
Keep working at same goal Modify the goal Pitch the goal and
using a different strategy start with a fresh goal
Re-write the Recovery Plan for this goal if needed!
9
Formulation

10
Form for planning and practice review- Provider(s) Date:
Client initials and age:
Session #/how long in treatment with you?
Client’s recovery goals: what does client really want to work on?
What are the client’s strengths and supports?
Symptoms/behaviors that interfere with meeting goals?
Current stressors / Substance use:
What would you like help with? Question for today’s consult
What have you tried so far (attempted skills/action)? and what was the outcome?
What do we know about the client (indicate history, beliefs, behavior)?
History: any life experience that helps us to understand the symptoms and behavior?
Beliefs: What does client tell self that might affect the symptoms or behavior? How can we
help client to shape a positive, affirming belief about self?
Behavior: What does client do that helps or gets in the way of goals/values?
Consultation/team suggestions:
Action plan: Skill/strategy to practice:
Inter-professional strategy:

11
Options for interventions/skill to practice: Identify skills to practice with client
Teach about how thoughts affect emotions
Explore behavior choices/options:
Teach Emotion regulation skill:
Build on a strength/interest area:
Identify supports together (family, spouse):
Develop specific coping strategy for :
Come up with a strategy for learning about something together:
Other:
Provider Self-reflection and feedback: How did the practice go? What might you try differently next
time?

12
Making Sense Formulation
What Happened Before?
(Predisposing Factors)
What Happened? (Precipitating
Factors)
What Keeps it Happening?
(Perpetuating Factors)
What Might Stop It?
(Protective Factors)
Target areas (goals or concerns)
Values
Social Activity
Situation
Physiological Response
Thoughts
Moods/Feelings and emotional regulation methods
Behaviors- helpful and unhelpful
Underlying Concerns/Core beliefs/schemas (show links where possible thoughts, feelings, behavior)
13
Engagement Strategies

14
Engagement Strategy Check Sheet
Check off the strategies observed during the role-play or audio review. MHP=
Mental Health Provider
Helpful engagement strategies
Present √
Example
Comment
Observation
Chose a place that is comfortable for the client to talk
Socialized and inquired about areas of interest to the client
Actively listened and reflected content accurately (did not
over generalize or leave out important content)
Showed curiosity and interest- tried to learn more about
client’s experience
Congratulated client for successes and accomplishments
Affirmed client’s values and/or interests
Let the client lead by asking what he or she wanted to
work on- attempted to identify something important to
client that MHP and client could work on together
Let the client lead by asking for his or her views on what
steps to take next.
MHP checked for understanding of what the client was
trying to say
Asked the client for feedback about the pace of the
meeting and let client lead by adjusting the pace to fit his
or her requests
MHP Expressed reasonable optimism
MHP used appropriate self-disclosure
MHP used a normalization strategy: stress-vulnerability;
common experience; well-known person, etc.
Asked client to summarize what he/she learned today or
what was most helpful
Asked for feedback about what client liked/disliked about
the meeting today
Other: something you did that helped build the
relationship with the client (list):

15
Clinical and Adaptive Mode Comparison
Mode 1: Clinical mode (one person plays client; one person plays clinician)
•
What brings you in here today?
•
What are your main stressors, symptoms, problem areas or challenges that
you want to address?
•
What treatment have you received so far?
•
What are your main goals?
•
Where would you like to start?
Scan body- report out how you feel physically and emotionally

16
Mode 2: Adaptive mode (one person plays client; one person plays clinician)
•
To start, if you don’t mind, I would just like to learn a little about you. What
do you really like to do? What are the kinds of things that interest you?
•
When are you at your best? What do friends/family consistently say is your
strength? Would you mind telling me a little more about these areas?
•
What are your big dreams. What would you like to be doing in the next 2-3
years?
•
What gets in the way of reaching your goals/dreams?
•
I wonder how you would feel about us working together to help you move
toward one of your goals?
Scan body- report out how you feel physically and emotionally

17
What is Psychosis?
The word psychosis is used to describe conditions that affect the mind, where there has
been some loss of contact with reality
1
. About 1.1 % of the world population develops
this kind of condition. That comes out to about 3.5 million people in the US alone that
receive a diagnosis of “schizophrenia.” About 75% of those people begin to develop this
condition between the ages of 16 and 25 years old. In order to receive a diagnosis of
“schizophrenia” the person must have had experiences of psychosis for at least 6 months.
Sadly, about 50% of those who are diagnosed have not received any treatment.
Many people who develop psychosis get better faster when they receive treatment
early in the process
1
. With quicker treatment, folks can get back to work, school,
hobbies, and relationships more quickly. When psychosis becomes a factor in a mental
illness, it responds well to early identification and treatment.
Psychosis does not equal “crazy” or “violent.”
1
In fact, most people who experience
psychosis are more likely to be victims of violence rather than the perpetrators of
violence. Psychosis is not a result of anything a person does or doesn’t do well or right.
Physicians struggle to know why some people develop psychosis and others do not. We
do know that it seems to be a combination of genetics and environment. We also know
that undergoing a lot of stress can sometimes bring psychosis on.
2
It is important to know that psychosis is a symptom of an illness. Psychosis is not the
illness itself
1
. Psychosis can happen within mental disorders or physiologically based
disorders. Sometimes it happens with stressful but common events that anyone may go
through, such as grief, lack of sleep, drug reaction, or trauma of some kind. Almost all
human beings experience a misperception such as a cell phone ringing when it wasn’t, or
someone calling your name when no one was there. Most of us think nothing of it,
though by definition, that is experiencing something that never happened in reality.
About 6% of us will have a psychotic “episode” in our lifetimes, so the vast majority of
people who experience psychosis will get better and never have another episode. In fact,
less than 1% of people with a psychotic episode will go on to develop schizophrenia
1
.

18
Psychosis can involve up to 3 types of symptoms: positive symptoms, negative
symptoms, and disorganized symptoms
4
I.
Positive symptoms are defined as something that is “added” to thoughts, emotions,
or behavior that was never there before. These are called hallucinations and/or
delusions.
A.
Hallucinations are categorized in the following way:
1.
Seeing things that others don’t see (visual hallucinations)
2.
Hearing things that other people don’t hear (auditory hallucinations)
3.
Tactile hallucinations are when there is a feeling of being touched when
there is no external cause.
4.
Olfactory hallucinations occur when one smells something that has no
external cause. Often the smell is unpleasant or there is a sense the smell
is coming from the person him/herself.
B.
Delusions
3,
5
are fixed false beliefs that can be very frightening. This is when
someone has a belief that sounds possible but not plausible (fearing someone is
watching, fearing others want to hurt you), and when people have more
unusual beliefs that sound way out of ordinary. This becomes a problem only
when the delusion interrupts daily living and quality of life. There are different
common types of delusions and these include:
1.
Delusions of Paranoia or Persecutory Delusions (i.e., belief that one is
going to be harmed by an individual, organization or group),
2.
Delusions of Reference or Referential Delusions (i.e., belief that gestures,
comments, or environmental cues are directed at oneself),
3.
Grandiose Delusions (i.e., belief that the individual has exceptional
abilities, wealth, or fame),
4.
Erotomanic Delusions (i.e., a false belief that another individual is in love
with him/her),
5.
Nihilistic Delusions (i.e., a conviction that a major catastrophe will occur),
6.
Delusions of Grandeur: Feeling super important, feeling like one has
super powers, or is an important figure like a celebrity or Napoleon.
7.
Delusions of Control: the belief that the mind is being controlled by
outside forces
8.
Somatic Delusions (i.e., a preoccupation with bodily functions)

19
C.
Distorted perceptions
2
mean that the person is having difficulty making sense
out of what they are experiencing (seeing, hearing, feeling, tasting, or smelling).
You may be having a hard time with experiencing lights as brighter and more
colorful, sounds that are louder than what you are used to. It can be increased
sensitivity to background or white noise. These are all distractions that you may
have never noticed before, and normally, you would be able to ignore them
without any hesitation.
II.
Disorganized Symptoms
3
include not being able to be understood by others when you
talk, or finding it hard to organize thoughts and actions and to plan ahead. This is
sometimes called a thought disorder.
III.
Negative Symptoms
3
are those things that have been taken away from a person
(emotions, behavior). When negative symptoms occur, the person feels so tired or so
anxious or depressed that they really don’t want to move. The instinct is to isolate and
hide away, limiting social contact, limiting time outside, little exercise, often not eating
well or eating too much. It may look like apathy or laziness, but it is not. Negative
symptoms are part of the array of symptoms that are seen in schizophrenia, bipolar,
or depression.
Are there warning signs before psychosis occurs? Often there are warning signs and
could include the following
2
:
•
Drop in grades, job performance, or other activities
•
Trouble thinking clearly or concentrating
•
Suspiciousness or uneasiness with others
•
Decline in self-care or personal hygiene
•
Withdrawing from family and friends and spending a lot more time alone
than usual
•
Stronger emotions (anxiety or sadness) than usual or having no emotions at
all
•
Sometimes experiencing things as louder or brighter than usual.
Sometimes people experience all of these experiences. Sometimes people
experience only one or two symptoms. We don’t really know why that is.
It could be hereditary, physiological, environmental, or any combination.

20
What does psychosis feel like? This is a tough question because everyone experiences
psychosis in their own way. Often, there may be experiences such as
2
:
•
Feeling like your mind is playing tricks on you
•
Things relate to you in a special way – a way that no one else notices
•
Hearing people talking or criticizing when you can’t see the person who is
talking (the talking person is nowhere to be found)
•
Feeling like certain things are super important in some special way
•
Making tenuous connections between things that are not usually connected
How can one begin to manage the symptom includes the following
2
:
•
Getting good sleep
•
Taking medications prescribed by your doctor
•
Avoid use of alcohol and other recreational drugs
•
Sticking with a Dr and a therapist and develop a plan for recovery
•
Staying active through exercise and social engagement
•
Stay in touch with people who support you
•
Talking with family or some trusted person in your life about what you are
experiencing.
Does recovery happen? Yes!
1
Sometimes these symptoms come in waves, and in
between the waves, the symptoms can be very manageable. A lot of people find recovery
in good solid medical help and working with a counselor and/or case manager. Many
people can go back to having the wonderful and full life they want to have.

21
This handout was adapted from:
1
Retrieved from: SARDAA (Schizophrenia and Related Disorders Alliance of America),
https://sardaa.org/resources/about-schizophrenia/
(NAMI), February 24, 2021
2
Retrieved from: Stanford Psychiatry Web Page:
http://med.stanford.edu/psychiatry/patient_care/inspire.html
. February 24, 2021
3
Retrieved from SARDAA (Schizophrenia and Related Disorders Alliance of America),
https://sardaa.org/wp-
content/uploads/2015/08/Nami_Understanding_Psychosis_Booklet.pdf February 24,
2021.
4
Smith, L., Nathan, P., Juniper, U., Kingsep, P., & Lim, L. (2003). Cognitive Behavioral
Therapy for Psychotic Symptoms: A Therapist’s Manual. Perth, Australia: Centre for
Clinical Interventions.
5
The Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM–5; American
Psychiatric Association [APA], 2013)
22
Working with Thoughts and
Cognition

23
Aspects of Experience
Thoughts
Behavior Emotions
Curious
Driving a car
I got a letter from my probation officer
Listening to music
I was like so frustrated I wanted to hit something§
I couldn’t breathe I was so scared
The voices are loudest at night
Guilt
Someone told my sister that I was getting high
I think I’m feeling ok now
I want to stop talking now
Are you angry with me?
My heart aches, I can hear my pulse in my ears, my hands are clenched
Laughing
This is stupid
It’s always going to be this way
Breathing activity (e.g. Square Breathing)
I have to go shopping
Afraid
Demons

24
Overcoming Barriers to Getting Active: What got in the way of getting active for you?
Common unhelpful thinking styles: Ways of thinking and solving problems that often leads to
distress or prevents us from following our values and goals!
All or Nothing: Belief that a situation is “all
good or all bad”- no middle ground; no
variations.
This involves words like Always, Never,
Everybody, and Nobody. This assumes that
the thought is 100% true all the time. It a thinking mistake because
one instance would prove the thought was false. It is unhelpful
because it keeps our mind on the negative.
Jumping to Conclusions: Making
a quick decision without getting
all of the information.
This happens when we quickly
react to events before having all
the facts. It is unhelpful because
when inaccurate, it leads us to
feel worse and maybe take actions
that are not helpful. For example, if I assume someone is threatening
to me and it is not true, I may leave/avoid or react in anger that can
lead to problems.
Circular Sinking Thinking: Staying in the same
negative thinking loop over and over.
There is often the belief that spending more
time thinking about a concern will help.
However, more time does not necessarily lead
to more helpful outcome. For example, if
someone spoke rudely to you at the store and the thought stays with
you all day- “that was so rude and unkind, why would the person do
that?” Staying stuck on the thought only leads to more and more
distress. We sometimes refer to this as rumination or excessive
worry.
Emotional Reasoning: Believing
something is true based on a feeling.
For example, feeling fear and believing
there is danger even when there are
no apparent signs of danger around
Fortune Telling: Believing with great certainty
that we know what will happen in the
future.
For example, “I will never get a job”. Just
because a person has struggled to find work
in the past does not mean that they won’t find
work in the future. It is both inaccurate and likely to decrease my
motivation to look for work.
Catastrophizing: Assuming the worst possible outcome will
happen in a situation.
For example, preparing to the store and thinking-
“the car will break down and I will have to walk
home in the rain.”
Discount The Positive- Not paying
attention to positive information.
For example, a person may beat
themselves, “that job interview was
terrible”, but refuse to give themselves
credit for positive aspects of the
situation, e.g., earning the interview, making positive comments
during the interview, or receiving positive feedback.
Mind Reading: Belief that we know what others are thinking
without checking. In reality, we cannot know for sure what
another person is thinking unless we ask them. If someone looks
at you when you enter a store and you think, “they want to hurt
me”, it is important to ask ourselves, how do I know this is true?
Could they have that look on their face for some other reason?

25
Unhealthy thinking styles can create Automatic Negative Thoughts (ANTS).
Examples of common Automatic Negative Thoughts (ANTs) that get in the way of activity:
My mental health symptoms prevent me from achieving my goals.
I can’t figure out what is important to me.
I don’t think it is possible for me to achieve goals.
I am afraid to take a chance. It would be bad to fail.
I don’t have the knowledge to accomplish goals (I don’t know how).
I don’t have any support to change from family, friends and others.
My physical health problems get in the way. I am too tired or hurt too much!
I have failed before, there is no use trying again
I should be doing better in my life
I always screw things up
This is just too much for me
Things are out of control
I can feel it, something bad is going to happen.
Your own:
Your own:
Your own:
Discuss these automatic negative thoughts in group and talk about which unhealthy thinking style
matches with the automatic negative thoughts above.
It’s possible that we have been stuck in our own automatic negative thoughts for so long that we don’t
even realize we are having them. That makes it hard to identify them, and even harder to change them.
Fortunately, there is a good way to get from unhealthy thinking to healthy thinking….
26
What do we know about thoughts?
• Thoughts come and go
• Sometimes we think of things on purpose, other times thoughts just happen
• Thoughts represent ideas- they cannot hurt you
• Thoughts can be linked with distressing or uncomfortable feelings, sensations, and
memories
• Some thoughts are inaccurate or come from misinterpreting events and we sometimes
call these Automatic Negative Thoughts (ANTs)
So what are we to do? Check the Thoughts! Especially the ANTS!
Reasons to check thoughts:
1.
2.
3.
Daily Practice: Catching the thought:
Situation 1: “I am late for my appointment!!”
Thought: They will be so mad, I am irresponsible --- Outcome: Feel anxious,
tense, beat myself up
Thought: They may be upset, but will understand Outcome: mildly nervous,
prepare a reason for lateness.

27
The Three-Step Technique (3Cs- Catch, Check, Change)
STEP 1: What am I thinking that is upsetting or troubling me? (Catch it):
What is the Automatic Negative Thought (ANT)?
Where am I? (what is the situation?)
STEP 2: Is there a better way to think about this? (Check it):
• Reality check: Is this thought really true/accurate? Could I be miss-reading the
situation? (What is the evidence?)
• Is this thought helping me or holding me back? Is the thought upsetting me? (What
will happen if I keep thinking this way? Is there another way to think about this
situation?)
STEP 3: Chose a better way to think and act (Change it):
• What other things could I say to myself (positive, balanced thoughts) that would be
more helpful? How might a close friend advise me to change my thinking? Look at the
situation and yourself in a kind and gentle way.

28
Situation: someone cuts in front of you in the store
Thought: That is rude and insulting
Feeling: Angry, upset
Behavior: Yell at person
Use your imagination:
Situation: Picture a beautiful lake, warm sun, sitting in a comfortable chair
Thought:
Feeling:
Behavior:
Yo
u pick a situation:
Thought:
Feeling:
Behavior:

Situation: “No one said hi to me at the store”
Step 1: What am I thinking that is upsetting or troubling me? (Catch it):
List the ANTs (automatic negative thoughts): Nobody likes me; I’m always
alone; I should leave and go home.
Step 2: Is there a better way to think about this? (Check it):
Reality check: That's not true. There are people who like me, others in the
store may just be busy or focused on their own stuff.
Step 3: Chose a be
tte
r way to think and act. (Change it):
Better thought: I can smile and say hi to others and get my shopping done.
Catch the thought
Change the thought
Check the thought

30
Situation:
Step 1: What am I thinking that is upsetting or troubling me? (Catch it):
List the ANTs
automatic negative thoughts):
Step 2: Is there a better way to think about this? (Check it):
Reality check::
Step 3: Chose an effective way to think and act. (Change it):
Better thought:
Check the thought
Catch the thought
Change the thought

31
Daily practice:
1. Think
of
one
or
two
situations
this
week
and
practice
identifying
your
thoughts
in
these
situations
(
Catch
it
practice!
)
Situation
1
:
Thought: Outcome:
Thought: Outcome:
Situation 2:
Thought: Outcome:
Thought: Outcome:
2.
Pick a situation that was distressing or difficult and practice the 3Cs method
(use the Catch it, Check it, Change it Handout)
•
Catch the thought: What thought is troubling? What is the situation?
•
Check the thought: What would other people say about the thought? Is
there another possible explanation? What facts do I have (remember fact is
different from thought); When I thought this way before, was it helpful?
•
Change the thought: What is another way to think about this situation?

32
Alternative Explanations
What is the thought/belief:
The medicine is poison and will kill me!
How much do you believe it: 0 – 100:
How much does it bother you: 0 – 100:
Evidence supporting the thought
Evidence NOT supporting thought
Pulling the information, what do you make of this?
What is the thought/belief:
How much do you believe it: 0 – 100:
How much does it bother you: 0 – 100:
Evidence supporting the thought
Evidence NOT supporting thought
Pulling the information, what do you make of this?
What is the thought/belief:
How much do you believe it: 0 – 100:
How much does it bother you: 0 – 100:
Evidence supporting the thought
Evidence NOT supporting thought
Pulling the information, what do you make of this?

33
Alternative Explanations Activity:
You say “Hi” to someone at the store and they do not say “Hi” back.
Possible Interpretation
Likely Emotional Response
They don’t like me Upset and sad
T
he phone rings and when you answer, you hear the phone hang up.
Possible Interpretation
Likely Emotional Response
Somebody is pranking me Mad
Li
st you own recent example:
Possible Interpretation
Likely Emotional Response
Adapted with permission from Friedman-Yakoobian, M., Gottlieb, J., Hollow, L., Pinninti, N., Carther, C. (2007).
Cognitive Behavioral Therapy (CBT) guide for case managers: Client Workbook.

34
Working on Cognitive Model Practice
Part 1: Working with Thoughts Practice
Scenario: Client holding mouth; complains of pain. When asked to describe- “spirits are beating me up in
the face”. “Demons used to be nice and now they are mean”. There is noticeable redness and swelling
near jaw and under client’s eye.
One person role-play client.
Other person role play case manager or therapist.
Practice: Ask client to describe the experience, and your job is to:
Step 1: Practice getting a full description of the experience. Then stop and identify the components
below: Remember to stick with the concrete details and facts!
•
Experience/Situation
•
Thought
•
Feeling
•
Behavior
Step 2: Summarize concerns into the components above. Check with client to see if you understood the
client’s experience accurately (validate/accept – (“I hear and understand”). Consider the other ways to
think about the event with the client (the person may or may not be ready to hear alternatives, follow
the client’s lead).
Part 2: Working with Emotions Practice
Step 1: Client agrees to get help, but there is a fear of provider and/or need to wait a few days before
seeing provider.
Step 2: Identify one emotion regulation or relaxation strategy that may ease the distress
One person play the client
Other person plays therapist who teaches an emotion regulation strategy/self-soothing strategy
consistent with your scope of practice.
Process:
What was helpful/effective?
More comfortable working with thoughts or emotions? Flexibility of your thinking? What was easy or
hard about this for you?
What is your practice action plan?

35
Changing Troubling Thoughts
Practice: Pick a situation in your life where you identify an automatic negative thought and check the evidence
Situation:
Automatic Negative Thoughts (ANT)
How distressing is that ANT (0-10 with 10 being the
worst?
How much do you believe the ANT (0-10 with 10 being the highest belief)?
Evidence for Thought
Evidence Against Thought
Look at the above evidence:
1. Staying in the present moment
2. In a balanced way
3. With kindness toward yourself (and others)
Outcome - New Action Thought (NAT):
Action plan - How will I put this New Action Thought into place in my life?

36
De-Center means to look at things from more than one perspective.
And then to choose the perspective that is likely to be most helpful.
Distressing belief/experience: example “Knocking on door”
Perspectives=
•
“It’s bad, just ignore”; leads me to feel and do
OR
•
“Let me evaluate and decide”
o
ok to protect my space; not answer door ok with that (their issue not mine)
o
Answer door and be ok to say “no”- stand up for self (their issue not mine)
o
Answer door and respond to request if it is reasonable and I chose to help
Pick another situation that concerns you:
Suspicious/other thought=
Because of this thought I feel=
Because of this thought, I do=
What are the facts? (did I check all the facts?)
What would other people say (write down another person’s view or alternative explanation)
W
hat makes the most sense to think and do at this time?

Name:
Date(s)
37
Thought Record for Belief
Situation: Sees Mary walking down the street. Waves at Mary, but Mary doesn’t wave back
First Thought and Then alternative Thoughts Feelings Behaviors
She hates me
Sad
Avoid Mary; Back out of
social involvement
She doesn’t like me
Worried
Could ask Mary if she is mad
at me for some reason
She didn’t see me
Neutral
Say “Hi” to Mary next time
Practice First Thought
Practice Second Alternative Thought
Practice Third Alternative Thought

Name:
Date(s)
38
Thought Record for Belief
Situation:
First Thought and then Alternative Thoughts Feelings Behaviors
First Thought
Alternative
Alternative
Alternative
First Thought
Alternative
Alternative
Alternative
First Thought
Alternative
Alternative
Alternative
Name:
Date(s)
39
Thought Record for Belief
Situation:
First Thought and then Alternative Thoughts Feelings Behaviors
First Thought
Alternative
Alternative
Alternative
First Thought
Alternative
Alternative
Alternative
First Thought
Alternative
Alternative
Alternative

Name:
Date(s)
40
Thought Record for Belief
Situation:
First Thought and then Alternative Thoughts Feelings Behaviors
First Thought
Alternative
Alternative
Alternative
First Thought
Alternative
Alternative
Alternative
First Thought
Alternative
Alternative
Alternative

41
Pros Cons
Do ………
Behavioral
Experiment
• Maybe the boss could work with me.
• M
aybe the cameras could be off
sometime.
• M
aybe I could learn about why they
have the cameras are on.
• They’re gonna think I’m a weirdo.
• T
hey’ll notice that I might not be a safe
person and I might get fired.
Don’t do…..
Behavioral
Experiment
• They wouldn’t know that I have
thoughts or that I get anxious.
• T
hey wouldn’t treat me differently than
they do now.
• T
hey wouldn’t have that I might not b
e
a
ble to take of the dogs.
• They would have more faith in me.
• I would continue to worry about why
the cameras are on and why they are
o
n.
• I
’ll get anxious and leave or I’ll get fired.
360⁰ Pros and Cons

42
360⁰ Pros and Cons
Pros Cons
Do
………
•
•
Don’t
do…..
•
•
43
Working with Emotions

44
EMOTION CHART
Sad Depressed Disappointment
Apathy Grief
Anger Mad Irritation Frustration Rage
Happy Joyful Glad Cheerful Loving
Fear Anxious Panic Nervous Shaky
Guilt/Shame Embarrassment Regret Humiliation Disgust
Jealous Envious Hurt Discouragement
Lonely
Content Calm Compassionate
Grateful Curious

45
Mood Diary
Monday
1 2 3 4 5 6 7 8 9 10
+ Good things today:
- Bad things today:
Tuesday
1 2 3 4 5 6 7 8 9 10
+ Good things today:
- Bad things today:
Wednesday
1 2 3 4 5 6 7 8 9 10
+ Good things today:
- Bad things today:
Thursday
1 2 3 4 5 6 7 8 9 10
+ Good things today:
- Bad things today:
Friday
1 2 3 4 5 6 7 8 9 10
+ Good things today:
- Bad things today:
Saturday
1 2 3 4 5 6 7 8 9 10
+ Good things today:
- Bad things today:
Sunday
1 2 3 4 5 6 7 8 9 10
+ Good things today:
- Bad things today:

46
Mindfulness Techniques
Grounding Techniques:
Normally, “grounding” techniques are a mindfulness technique that is a guided process that instructs
the participant to take in information through the five senses. Often, it is taught as a “practice”, and
there is some, what I often call, mindfulness “fluff” to it. This can be inspiring to some, and offensive to
others.
When working with people who are panicked or are bordering on experiencing memories, simply giving
them concrete instructions works best. But the participant must have had the instructions prior to the
urgent incident taking place.
Education for Grounding: Simply describe “grounding”.
“Grounding is a technique that helps to keep someone in the present moment. Lots of times, we
get lost in memories or thoughts, and we can get upset by them. We get so lost in them that we find
ourselves right in those memories and thoughts instead of being right here in the moment. Grounding
helps to simply keep us in this moment. We do this (I’ll say “I do this” because it is true that I do this) by
looking at the place I am in – the walls, the floor, the colors, the sounds, the sights, even the smells, and
maybe even the touch of things. Feel the wood of the chair frame you are sitting in, listen to the music
playing in the next room, notice what colors are on the walls. Describe the pictures on the walls. I’m
going to remind you to breathe as you do this. Maybe even breathe with me and match my breath (then
match their breath, and begin to slow the pace down a bit, if that is necessary). Remind yourself of
where you are, when you are, and who you are with. Say those things out loud.”
As I am asking them to feel, see, touch, and smell all these things, I ask them to very briefly
describe them to me (The walls are blue. The arm of the chair is smooth wood or metal. The door to the
room is made of wood. I smell rain in the air. etc.). Breathe with them until their breath slows down, and
they can calmly state where and when they are and can identify you.
It is best to teach them this skill when things are going well. Practice this skill when things are
going well. To slow down their own breathing when they are alone, they can put their hand on their own
belly and feel how quickly they are breathing and attempt to slow the breath by that simple feedback
method. Perhaps at the beginning of every meeting for a quick minute or two. That way, when panic or
terror begins, they have a method that they have practiced and are familiar with.

47
Relaxation Techniques: Isn’t it hard to relax when that is exactly what you are trying to do? I think so
too. That makes relaxation very hard to teach. Relaxation is about giving one’s self a rest. We hold our
bodies so rigidly when we are anxious. There are many ways to teach relaxation and many aids to help
guide one through a relaxation technique.
1.
Find a relaxation technique that you like and share that with your client
2.
Sometimes, relaxation is more about giving your mind a rest than your body
a.
I often play piano or guitar to relax
b.
Sometimes I watch TV to relax
c.
Sometimes a listen to relaxing music
d.
Sometimes I practice yoga – relaxing yoga
e.
Sometimes I paint to relax
f.
Walking
g.
Playing with my dog
h.
It’s not always about letting go of muscle tension, it can be about letting go of all the
thoughts and memories and chores and judgments we have going on in our heads.
3.
Education for Relaxation: Sometimes relaxation is about letting go of muscles:
a.
Preparation: “Sit in a chair, or lay down on a mat or comfortable place and pay
attention to your breathing. Attend to your breath moving in and out of your body,
paying more attention to the out breath than the in breath. Attempt to make the
out-breath longer than the in-breath (this cues the parasympathetic nervous system
to go “online” and will naturally calm down the central nervous system without
conscious awareness.) As you breathe out, allow your muscles to let go and rest.
With each out-breath, allow your muscles to let go even more. Feel the heaviness of
your body in (the chair, sofa, bed, yoga mat, etc.).
b.
Mindfulness: Just rest for a moment and feel yourself breathe. This is a kindness you
are giving to yourself, to relax, to let go of your tension for just a moment. When
you find yourself thinking of other things, congratulate yourself for catching that,
and gently and lovingly bring yourself back to letting go of your muscle tension with
each breath.
c.
Closure: When you are ready, begin listening to the sounds in the room, feel the
clothes you are wearing, feel whatever it is you are laying on, hear yourself
breathing, Remind yourself that you deserve to have a rest and rejuvenate yourself,
and gently bring yourself back to the moment, ready to go on with the rest of your
day.
4.
Progressive relaxation can be helpful (there are guides everywhere) but the process can
often be so long that it is hard to pay attention to. Give it a try if you’d like to. It can have
profound effects if one has worked up to the task of relaxation periods of longer than 15 to
20 minutes at a time.

48
Breathing Techniques:
Posture: A few words should be said about posture. With breathing (as with mindfulness when we come
to it), posture is important. The idea is that we want to pair a sense of dignity and honor to the
experience of being in our bodies, and being in our bodies in the here and now. Having a fairly upright
posture is best. I suggest having feet on the floor, or legs gently crossed if the participant is sitting.
Shoulders and hips square to the body and relaxed. Jaw gently dropped. Hands on thighs palms down.
Sitting in a dignified manner, as if one were the King or Queen of this particular spot on the earth. Sitting
with honor and dignity begins to introduce a felt sense of honor and dignity. No manipulation of the
breath is necessary.
Visibly work with them on posture – practice the posture with them yourself. Do this each time. Make
these associations frequently, and clients may begin to follow your lead regularly.
Square Breathing:
1.
Breathe in to the count of four
2.
Hold your breath to the count of four
3.
Breath out to the count of four
4.
Do this four times
Mindful Breathing:
1.
Breathe normal breaths. Count each out-breath only. Count up to 10 out-breaths. Begin again if
you need to.
Or….
2.
Sit quietly for several moments. Say to yourself as you breathe normally…
“I am breathing in” – when you are taking an in-breath
“I am breathing out” – when you are taking an out-breath
With any mindfulness technique such as breathing, always put into the directions or instructions that
minds wander, and that is natural and normal. Do not be dismayed by constant mind wandering. On the
contrary, congratulate yourself that you have done exactly what mindfulness practice is designed to do
– c
atch ourselves doing something other than what we are targeting, so that we can gently and
compassionately bring ourselves back to our frame of reference – our breathing. Excellent job!

49
Mindfulness Techniques and Working with Voices
These mindfulness activities are particularly good for helping clients to manage dealing with voices. Give
instructions and practice with clients or have them practice with you. Then process the experience with
them. Have them practice daily. Motivation, effort, and practice will help these particular activities work
proficiently. The name of the game here is PRACTICE.
Sub-vocalizations:
There is something about sub-vocalizing that interrupts the process by which auditory hallucinations
seem to be produced. This can work for intrusive memories and thoughts as well. Simply reading a
book to one’s self does not seem to work. Reading it out loud does seem to work.
1.
Read a book out loud
2.
Read a book at whisper level
3.
Read to someone
Look Point Label:
Have them look around the room or area where they are and find an object. Have them point at it.
Have them say the name of it out loud. Do several rounds of this. This pulls them back into the
present moment.

50
Mindfulness Practices and Survey
Helpful
Have used the
skill outside of
group
Not helpful or
don’t remember
Session 1
Mindfulness to Breath
Square Breathing
(4 in; hold for 4; 4 out; 4 times)
Session 2
Mindfulness to Thoughts
Using words to notice changes
In thoughts and physical experience
(Peace, Loss, Lama Spit, Compassion)
Session 3
Mindfulness to Listening
Using music to identify changes in
body sensations and emotions
(Moonlight Sonata, Jazz, Choir)
Session 4
Mindfulness to Touch (Grounding)
Examining a stone – noticing all aspects
of the stone – color, texture, size, turning
it over, being curious about the stone
Session 5
Mindfulness to Eating (Savoring)
Used raisin or “craisin”, allow it to be in
your mouth without chewing, feeling the
texture, biting it without breaking into it
savoring the flavor as you finally bite;
Chew with conscious deliberation

51
Helpful
Have used the skill
outside of group
Not helpful or don’t
remember
Session 6
Mindfulness to Gratitude
Share with another person what
you have learned from them – what you
are grateful about what they have taught you
Session 7
Loving Kindness
“May I be filled with loving kindness;
may I be held in loving kindness”
See handout – Session 7
Session 8
Mindfulness to Thoughts
Relax into breathing
Focus on breath
When thoughts arise, as they always
will, label them and place them on
a cloud to pass by, or on a leaf
in a river to float down the stream
Session 9
Mindfulness to Sight
Browse the paintings in the hallway
share with a friend the items that you
enjoy or don’t enjoy, or have feelings or
thoughts about – describe what came
up for you, listen to what came up for them
Session 10
Mindfulness to Discomfort
Focus on your breath
Scan your body from head to toe
Notice any tightness or discomfort
Open up space inside your body for
that experience to begin to dissipate
and lose its tenseness.
Send imaginary heat or light to that
area to relax the sensation
Extra
Progressive Muscle Relaxation
Starting with the top of your head, gently
squeeze and then release each major muscle
group: scalp, eyes, jaw, neck, shoulders,
triceps and biceps, forearms, hands, chest
muscles, abdomen, buttocks, thighs, shins and
calves, feet, and finally toes. Feel the warmth
coming into your muscles when you release
the squeeze. Relax

52
Emotion Regulation in the Brain
Definition of Terms
INSULA
• The Insula helps combine physical experience of the body and the emotion experienced –
helps us to be aware, emotionally and physically, in the present moment
• Controls autonomic functions through the regulation of the sympathetic and
parasympathetic systems – works for homeostasis
• Regulates the immune system
AMYGDALA
• Responsible for perception of emotions
• Stores memories of events and emotions so we can recognize similar events in the future
Both the amygdala and the insula are vital in the experience of shame
ALEXITHYMIA
• Multidimensional construct
o Difficulty identifying emotions
o Difficulty describing emotions to others
o Difficulty appraising their bodily sensations
o Constricted imaginary processes
o External locus of control (externally focused)
• 2 subcomponents of Alexithymia
o Cognitive-emotional component (verbalizing & analyzing)
o Subjective-Emotional component (emotionalizing & fantasizing)
• Individuals with schizophrenia tend to score very high in the construct of alexithymia

53

54
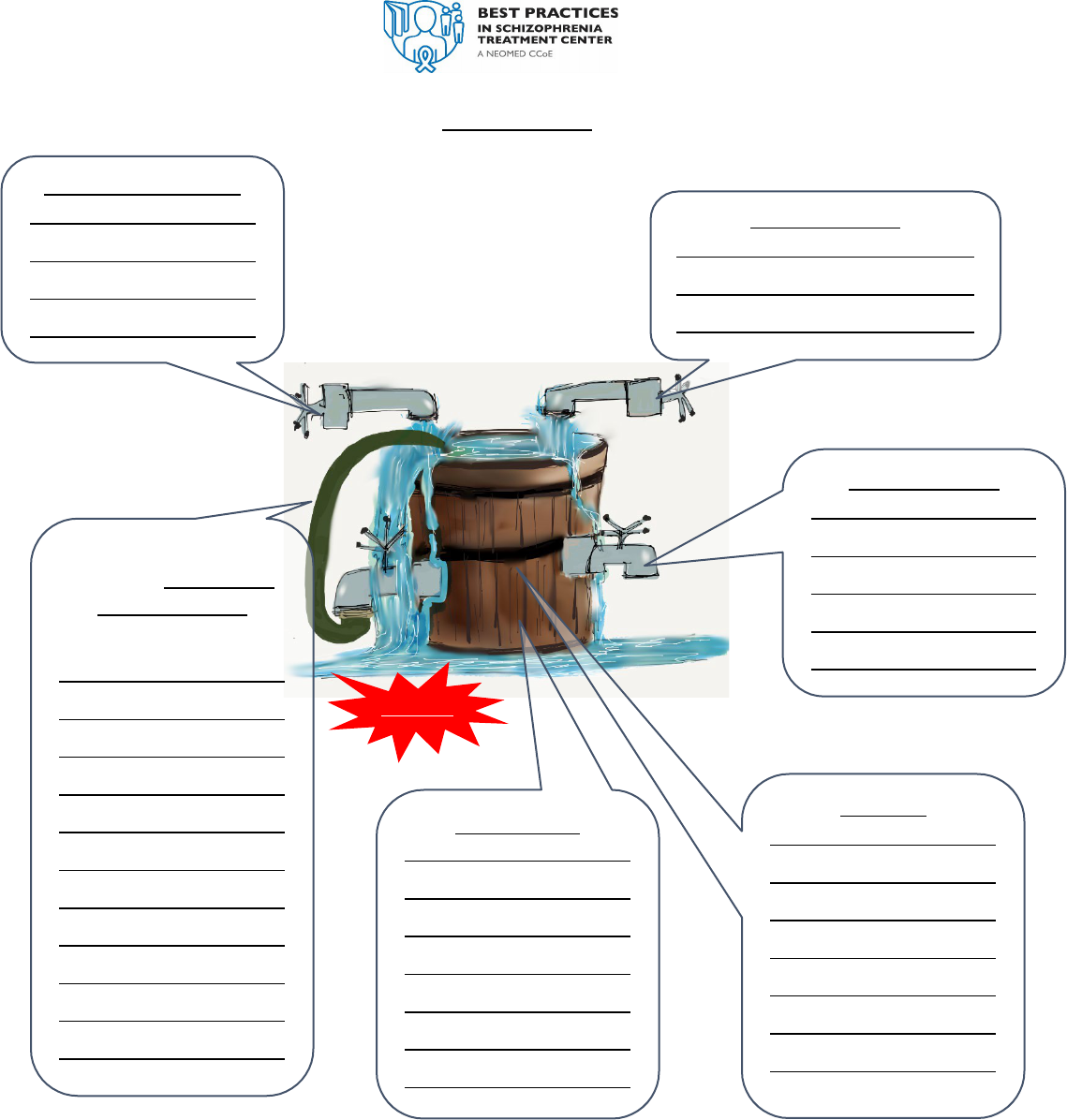
The Stress Bucket
Everyone experiences stress at some time in their lives. It’s part of being human.
Sometimes, we will choose a path in life that is stressful, but we choose it because we believe that
the decision is a good one for us. We believe it will keep us safe, well, and happy. Even good
changes are stressful sometimes.
• Getting a new job
• Going back to school
•
Moving to a new home
• Starting a new relationship
• Ending a toxic relationship
• Beginning counseling or treatment
Can you think of times when you have made a decision that was “good for you” to make, but was still
stressful?

55
The Stress Bucket Model shows that too much stress is not good for our bodies, no matter who
we are or what we struggle with. When we get overwhelmed with stress, symptoms begin to
show up whether they are symptoms of depression, anxiety, diabetes, getting a cold, irritability,
and the list could go on and on. This model shows that symptoms arise for anyone.
If you can imagine stress as water that flows into a bucket, it’s easier to see how stress affects
us. It’s like water flowing into a bucket, and there’s nowhere for all that stress to go.
Water (or stress) begins to fill the bucket, the bucket becomes full of stress (or water). After a
while, there’s no more room in the bucket and it begins to overflow. When that happens, we
begin to have some symptoms related to that stress. This can include:
• Panic or anxiety
• Depression
• Hallucinations (auditory, visual)
• Sleep problems
• Headache, stomach ache, back pain
• Vulnerable to colds and flu
• Jittery or irritability
Vulnerabilities
Vulnerabilities can make our bucket
leaky, and the water, or stress,
begins to find another way out, but
usually not in an effective way. These
can increase our stress too.
Vulnerability can be thought of what makes us more fragile to stress. The more vulnerable we
are, the more likely we are to feel the stress. Vulnerability can be thought of as the size of the
bucket.
Some of us have a smaller bucket, which
means that it won’t take much stress
before the bucket overflows.
Some of us have a big bucket, which
means that it can take lots of stress
before the bucket overflows.
+
56
Daily Practice
Interpersonal Stressors
General Stressors
New Coping Skills
Unhelpful coping
strategies. What do you
need to work on?
Symptoms
Vulnerabilities
Resilience

57
When we are not sure how best to manage the stress, we do whatever we can to cope with it.
If we haven’t learned healthy ways to deal with stress, we will use ineffective ways to cope,
like…
• Drug or alcohol use
• Yelling or getting into fights
• Feeling so hopeless that we stay in bed
• Anxiety that is so high that we begin to fall into circular sinking thinking
• Miss appointments with therapist, case manager, or physician (avoiding because the
transportation is hard, the doctor might not say what we hope they will say, not really
feeling like sharing with my counselor or case manager).
• Just not paying the bills because we are afraid to look at them
Are you aware of ways of coping you use that haven’t been very effective at reducing stress,
and in fact, may increase your stress, adding more water to the already full bucket.
Using ineffective coping skills like drug use, alcohol use, avoidance, staying in bed all day, or
watching TV, works in the short term, but not all the way, and after a while, our bucket begins
to leak anyway. It’s just like hooking a hose from the bucket, and putting it right back in at the
top again. The hose doesn’t even help with our vulnerabilities either.
But what we can do is to use some effective coping skills. That allows the stress to come out in
a way that we choose.
Coping Skills
The faucets in the bucket represent coping skills. It’s possible to learn to manage the
amount of water (stress) that stays in the bucket in a variety of ways:
• Lower the number of stressors
o Reduce your workload if possible
o Ask for help around the house
o Get some extra rest if you need to
o Improve sleep (which is different than “get some extra sleep”

58
• Improve coping strategies
o “Catch it, Check it, Change it”
o Grounding
o Mindful breathing, and other mindful activities
o Taking medications regularly if that is on your treatment plan
o Talk to your counselor or case manager if you need to
o Monitor your emotions
o Exercise
• Build up resiliency – work with the strengths you already have. Think about some
effective and healthy ways of behaving that you already demonstrate that have
been helpful to you.

Stress Bucket
59
Daily Practice
Interpersonal Stressors
General Stressors
Begin to work on and
change the unhelpful
coping strategies. What
do you need to work on?
Resilience
Symptoms
Vulnerabilities
New Coping Skills

Stress Bucket
60
Interpersonal Stressors
Daily Practice
General Stressors
Resilience
Begin to work on and
change the unhelpful
coping strategies. What
do you need to work on?
Symptoms
Vulnerabilities
New Coping Skills
61
Working with Behavior

62
Behavioral Experiment
Prediction
What is your prediction?
What do think will happen?
Experiment
What experiment might test this prediction?
What safety behaviors need to be reduced?
How would you know if your prediction came true?
Outcome
What happened?
Was your prediction accurate?
What did you learn?

63
Behavioral experiments: Setting up the Investigation
We have learned that our thoughts are different from facts
Remember: if I think “chair will break” does not mean that it will break
We have learned that there are many reasons why our thoughts may not be totally 100%
accurate
Remember: unhelpful thinking habits
We have also learned to identify the thoughts that bother us and to check those thoughts by
• Coming up with alternatives
• Using a pie chart to see how strongly we believe different thoughts
• De-center and see how other people see the situation.
Sometimes we may also need to get additional information to check our thoughts. It is like
being a detective whose job it is to evaluate the accuracy of certain thoughts.
• Who is your favorite detective?
• How does that person get to the facts or what really happened?
See below for the most common ways we can address our thoughts by being our own “inner
detective”.
Research: Look up information from a reliable source or take a survey of those you trust
Experiments: When a detective has a good theory, he or she may set up an experiment to
check out his or her theory. See below for ways to investigate thoughts

64
The Investigation Analysis Worksheet 1
What is the troubling thought or experience?
What is important about this thought or experience?
How sure am I about the accuracy of my belief about the thought or experience?
Is there another way to think about this situation?
What additional information would help me with this troubling thought?
Where would I find information that I need or want?
Can I do research from resources that are objective?
Is it testable in some way?
Can I take pictures?
Can I make a recording?
Can I ask questions with people I trust (taking a survey)?
Write out your experiment.
What is the expected outcome of my experiment? What would it mean if your thought was
confirmed or disconfirmed?
What is the actual outcome of the experiment?
What do you conclude from going through these steps?

Investigation Analysis Worksheet
65
Thought
Belief %
Alternatives
Belief %
Investigation
Research/Experiment
Expected
Outcome
Actual
Outcome
New Thought
People are
monitoring me
– I answer the
phone and the
other party
hangs up.
90%
Could be wrong
number
Could be an
auto-dialer from
a solicitor
10%
10%
Research
Look up info on
telemarketing
Look up info on auto-
dialers
Ask other people I trust
if they get hang-up calls
and what they think
about them.
Not sure what I
will find with
the research
Still get hang-
ups, but I have
new info on
telemarketing
and auto-dialers
Could be an
auto-dialer
50%-50%
Things in my
home have
been moved
since the last
time I was here
90%
Forgot where I
left things
Pets moved
them or
knocked them
over
Furnace air or
wind from the
window
10%
10%
10%
Experiment
Set things in specific
places
Take a picture
Cage the pets for a day
GO OUT for period of
time; return
Things will be
moved
Things didn’t
move
Sometimes I
just don’t
remember
where I put
things
Maybe it was
the pets
Meta-thinking
(Alternative
explanations)
Pie Chart
(List alternative
explanations)
De-Centering
(Get another’s
perspective)

Investigation Analysis Worksheet
66
Thought
Belief %
Alternatives
Belief %
Investigation
Research/Experiment
Expected
Outcome
Actual
Outcome
New Thought

Investigation Analysis Worksheet
67
Thought
Belief %
Alternatives
Belief %
Investigation
Research/Experiment
Expected
Outcome
Actual
Outcome
New Thought
68
Working with Voices and
Hallucinations

69
Voice Diary
Situation
Where are you?
When? Day and Time?
What are you doing?
Voice Present
Yes/No
Voice Content
What did voice (s)
say?
Distress Level
1(None)-10
(Extremely
Distressed)
Response
What did you do
(behavior)?
Outcome
What happened?
Voices- stop or continue?
Distress- go up or down?
Re-rate (1-10)

70
Some Ideas about How to Cope with Voices
Frustrating the Voice by Repeating Everything:
- Some voice hearers have found it helpful to repeat to themselves everything that the
voice says, word for word, in your mind. For many people, this causes the voice to
stop, or at least become calmer. A variation on this has worked when the voices
seem very loud: when you repeat to yourself what the voice says, just slowly reduce
the “volume;” this tends to lead to a lowering in the volume of the voice itself.
Using Earplugs:
- Putting an earplug in just one ear has helped a lot of people, at least for a little
while! Experiment with using either the plug in either your left or right ear. If it
doesn't work, try taking the earplug out: for some people the voices stop when the
earplug is taken out!
Figuring out what is, and what isn't, actual sound waves
- If you are often unsure whether you are "hearing voices" or just hearing say the
neighbors talk, or the TV, you can try the following exercise. Get a tape recorder.
When you are starting to wonder what you are hearing, start recording. While it is
recording, maybe just for a few minutes, make a guess as to whether what you are
hearing is going to show up on the tape as being normal sound. Then play the tape
back and see whether you were right or not. Over time, you should be able to get
better and better at guessing.
Focusing on the voices
Anything you do to study the activity of the voices fits in this category.
- For example, one method is to notice each day how intense and disruptive the
voices were that day, and to give them a rating on a 1 to 10 scale. You can even
collect more detail and rate them on how intense they are in each hour. This
information could be kept on a chart which might allow you to see when the voices
become stronger and when weaker.
- Another method of focusing on the voices might be paying attention to triggers:
things that seem to occur right before the voices get stronger. You can then work on
better ways to cope with those triggers, so they don’t bother you so much.
- Studying the voices. This might include asking them questions about themselves,
while noticing any inconsistencies and asking about those as well. You might ask
them how old they are, what benefit they get from pestering you, what they like to
do for recreation, anything that crosses your mind. By actively studying and by
asking questions you are taking the initiative, rather than letting the voices have all
the initiative.
Adapted from Ron Unger, 2018 blog; https://recoveryfromschizophrenia.org/cbt-for-psychosis-t
rauma-
psychosis-handouts/2097-2/

71
- You can write down exactly what the voices say, and then notice any themes, any
issues the voices are preoccupied with.
Distraction. (avoid over-use of distraction, as those who cope best don’t seem to focus on
using this method.)
This category includes anything you do to divert your attention away from the voices. Some
possibilities include:
- Going out for a walk, doing some shopping, travelling around on public transport as a
form of diversion than without serious intent to travel to any particular place, going
out for a drive or even visiting a transport hub like an airport or busy railway or
station..
- Doing routine domestic chores at home, washing, ironing, cleaning or gardening etc.
- listening to a radio, a walkman or stereo (music without words might be better if
hearing words in the music gets voices going for you).
- It might be a good exercise to create your own list of things that you particularly like
to do as a reminder that you refer too when you having a particularly hard time with
the voices.
Concentration
This includes anything you do that really requires you to concentrate on something other
than the voice.
- reading, studying (but not if studying is a major stressor for you,) writing a journal or
diary, or creative writing, doing art work or sculpting or something related, putting
together models, jigsaw puzzles, repairing things at home or maybe at someone
else’s place, Playing chess, shooting pool, going to a bowling alley, playing racket
sports, playing a musical instrument e.g. guitar, drum, violin or keyboard instrument
synthesizer: it could be things like singing specific tunes or songs, even attending a
choir etc.
- Another form of concentration activity is what is termed SUBVOCALISATION.
Essentially this means doing specific tasks in your head that you might otherwise use
your mouth for. Examples of this method would be ‘counting’ (in your head up to
100 rather than aloud), or singing a song under your breath
Physical Exercise
- like taking a walk or a bike ride, working out at the Gym, Yoga, or swimming.
Physical activity can improve mood as well as help calm the voices.

72
Social Activities
This means undertaking activities that involve others.
- You might take time to speak with a partner, a close friend, or even a sympathetic
worker, if you for example live in some kind of formal residential setting.
- Telephoning a friend/s
- Visiting (fairly supportive) friends or relations who are fairly supportive to you even
they may not necessarily understand your experience.
- Attending groups, such as peer support groups such as one for voice hearers, or
joining a hobby/activity groups.
- Be careful to avoid social situations where people are likely to be “negatively
critical.” Experiences with people with these attitudes frequently results in feeling
worse. Instead, seek out people who know how to be constructive, people who can
see some good in you and help you see how to build on that.
- Also, don’t expect too much out of yourself in social situations. No one can please all
of the people all of the time, and if you try to make yourself please everyone, you
can make yourself miserable!
THINKING (cognitive approaches)
Thinking (termed Cognitive) strategies means using your thoughts in a self-aware way to
challenge or in some way diminish the sense of voices having power over you.
- ‘Reality testing’ The voices may be saying something about your friend or partner,
for example, saying that your friend is angry at you about something. Providing that
your friend is understanding and are not likely to take offence, you might try asking
your friend directly if this is true. You may have to be cautious about the content of
what you wish to check out with person the voices are speaking about, as some of it
may just be too intrusive or personal and may actually cause offence! And it may be
the voices just want to get you into trouble or bring trouble in your friendships or
with the people the voices are attacking.
- Negotiating ‘TIME OUT’ with the voices or otherwise postponing (delaying) listening
to the voices. In exchange for giving the voices your positive attention say for a half
hour or an hour you ask them to go away for half or a whole day. You may have to
experiment with this awhile to get some effect. Its’ like saying I will reward you with
positive attention for a while if you then shut-up for the next four hours or so. Or you
say if you go away now I will give positive attention towards the end of the day say
5pm etc.

73
- Providing you don’t feel too frightened of the voices you could practice bringing
them on then dismissing them: this can really work for some people and build up
their confidence over controlling some of the voices.
- Thinking positive thoughts of yourself. Thinking positive thoughts about yourself
when the voice are around (voices are often negatively critical), perhaps writing
something positive about yourself, your achievements or what you might want to do
in the future etc. You may have a portfolio (or album) containing mementos of things
you achieved in the past, it can be helpful to look at these as a way of recalling
positive aspects of your life.
- Changing what we think about the voices. Changing the way we think about the
voices may be more difficult to do on your own and it may be better to speak to
someone possibly trained in some form of therapy like Cognitive Behavioral Therapy
(CBT) to help with this. Sometime the meaning we put on our belief of voices is
termed ATTRIBUTION. Psychological therapies like CBT as previously mentioned can
be used to help us to more objectively weigh the evidence for and against particular
ideas about the voices: therefore, help us REATTRIBUTE our ideas about the voices:
that is changing our beliefs about the voices. This can be especially helpful if we find
ourselves stuck with certain ideas about the voices which continually distress us and
may not be true.
Getting to know the emotions behind the voices
- If you watch voices carefully, you might notice certain voices that pop up at certain
times, or say particular kinds of things at certain times. For example, it may be at
times when you are alone, or when something embarrassing or unpleasant has
happened. Try to observe and appreciate what you are feeling at the time. Focus on
the emotion you are feeling as what is really going on; you may find the voice
becomes less important as you give yourself permission to directly feel the
unpleasant emotion.
- Once you know the emotions that stir up the voices, you can also work on
encouraging counter-emotions. For example, if voices are stronger when you
are bored, work at making your life more interesting. If they are stronger
when you are feeling disgusted with yourself, work on ways of increasing
your self-respect and reasons for respecting yourself. This can be an
extremely important way of fighting voices!
- Imagining that you are the voice & try to understand why you would want the say to
your “self” the things the voice says. Try to get inside the “head” of the voice, the
way you might try to get inside the "head” of a character in a novel or movie,
understanding its emotions, drives, and strengths and weaknesses.
- Once you understand the life of the voice better, you can start wondering
about what it needs, and even showing care and compassion for it. For
example, maybe it bothers you because it is scared, and you could imagine

74
ways to help it find peace. Or maybe it is very rigid, and you could look for
ways to help it be more flexible. This is not about giving in to the voice at all,
but is about helping to give it what it really needs instead of what it may
demand from you all the time.
Questioning the Voice:
- Voices love to act like they are big authorities, and often people get sucked into
believing them! You can help yourself by questioning their authority. Example: a
voice is disturbing you by saying that you are evil, and you don’t know why the voice
is saying this. You can challenge the voice, and say “Prove it!” Either the voice will
shut up, or it will have to try to prove it, and then you can dispute whatever “proof”
it comes up with.
- Voices also like to give themselves fancy identities, such as claiming to be famous
people or important spiritual beings, etc. You can dispute this by thinking of some
question that you yourself don’t know the answer to, but that the voice should know
if it really is who it says it is. Get the voice to answer the question, and then look up
its answer to see if it got it right.
Using Art
- You can draw the voices, or sculpt them, or make some other representation of who
or what they seem to be. This can help you deal with the voices in a new way.
- Another approach, perhaps more advanced, is to "take the role" of the voice, or to
mimic it, the way an actor or actress takes on the role of a character in a play or a
movie. For example, if you have an "evil voice" you could play the role of this voice
the same way that an actor plays the role of an evil character. If the "evil voice" tells
you to kill yourself, then when you play the role of the voice you would pretend to
be telling someone to kill themselves. You can even play this role in an exaggerated
way, being more dramatic and "evil" than the voice usually itself is. You could try
this with your therapist if your therapist agrees, or practice in front of a mirror. This
method can help you step out of the role of feeling like a "victim" of the voice. It will
only be helpful if you feel ready for it and if you can keep it clear in your mind that
you are just acting an evil role, not being evil or going to do evil things yourself.
Seeking out positive and constructive voices while tuning out voices that tend to be
negative:
- This involves, first, making an effort to distinguish which voices are really offering
something constructive versus those that are just causing trouble. Then, for
example, when you hear a negative voice, you can instead seek out the company of
one of your more positive voices. (One way of calling it up might be just being
curious about what the positive voice might say, or imagining what it would say, or
remembering the kinds of things your positive voice said in the past.) You might
even try asking the positive voice for advice on how to deal with the negative voices.

75
- If you tell someone, "don't think about elephants," it's elephants that they'll think
about. So don't worry about trying to "not hear" destructive voices; instead just
focus on paying attention to constructive ones.
Seeking out positive and constructive thoughts & activities while tuning out voices that
tend to be negative:
- Any focus on something constructive, that makes you feel good about yourself and
what you are doing in the world, can help create good feelings that protect you from
the voices.
- Remember that to really make the constructive things you are doing count, you have
to give yourself credit for them. One way of doing this is to write each day in your
journal about what you did that day that was constructive, and perhaps what you
plan to do in the next day.
Using imagination or visualization to protect yourself.
- For example, you might imagine a sort of "halo" or protective light around yourself.
Or, you might find an inner guide who can give you advice or help defend you from
the voice. You can imagine whatever it might be that you would need to overcome
the voice: there are no limits on what you can imagine! You might start out thinking
that the voice is more real than your imagination, but remember that the voice
depends on you paying attention to it and believing that it has power: if you pay
more attention to and put more belief into what you imagine that is protecting you,
the voice will lose power.
Learning to quit expecting the voice:
- This method takes advantage of the fact that people tend to hear the voices they are
expecting to hear. If you create a counter-expectation, that counter-expectation can
eventually overpower the expectation to hear the voice. For example, suppose you
are used to hearing voices and getting preoccupied with them when you go home in
the evening. Instead, think about what you would like to be preoccupied with in the
evening. For example, maybe you would rather be focused on some good music, or
a novel you are reading, or working on a project. Focus on expecting that from
yourself, and if the voices try to intrude anyway, expect them to become less
important as you focus on what you really want to pay attention to.
Notice how the voices are not all that original:
- To do this, you need to keep 2 written records of what happens when you are in a
distressing situation. In one record you write down the thoughts that come to you
automatically about yourself when you are in the distressing situation. In the other

76
record you write down what the voices say when you are in those situations. Later,
you can look at these records and see how much they are the same or different.
Reframe what the voices are saying as something positive
- Using this method, you assume that the voices are really trying to help you in some
way, though perhaps they are misguided or overly enthusiastic in what they are
trying to do. For example, if the voice tries to convince you that everyone hates you,
you might reframe it as trying to make sure you aren't overly self-confident. If the
voice wants you to kill someone, you might reframe it as the voice wanting to make
sure that person doesn't take advantage of you. If the voice wants you to kill
yourself, you might reframe it as the voice wanting to save you from a distressing
situation that it is worried will be too painful for you to endure. By finding a possible
positive intention in what the voices say, you can then focus your attention to
handling those concerns, and you can even thank the voice for its concern and ask it
to help you. For example, you can tell a voice that wants you to kill someone that
you appreciate its desire to not let you be taken advantage of, that you do not want
to go so far as to kill the other person, but that you are open to other suggestions
about how to protect yourself from this person. When you reason with the voices in
this way, you might find that a healthier dialogue begins inside you.
Reframe hostile voices as helping you get in touch with difficult feelings:
- This one is a little tricky but potentially very helpful. Hostile voices can be verbally
abusive, and can even encourage people to give up on themselves or hurt
themselves or others. People can then get into long and emotionally exhausting
battles with these voices. This method asks you to try something a little different.
- Instead of fighting back against the hostile voice, imagine that the voice has
won, that the voice has all the power and that it has already hurt you in the
ways it is trying to hurt you. How does it look or feel to you that this has
happened? What is most difficult to you about this feeling?
- What do you need when you are wounded or overwhelmed like this?
- Once you get in touch with the sad or wounded feelings, then let yourself
notice that there is also a healthier you that can provide some of what you
need at this moment. You can then focus on giving yourself some of what
you need, you can practice self-comforting.
- The magic of this method is that you quit fighting with the voice, by focusing instead
on how it feels to be the victim of the voice. (But you do it without actually hurting
yourself - for example if the voice wants you to cut yourself, you focus on what it
feels like to be a person forced by someone to cut themselves, how it feels to be sad
and overwhelmed, you don't actually cut yourself.)
- The notion behind this method is that voices often try to get people to feel horrible
or vulnerable feelings which the person has disowned: by accepting and owning the
bad feeling, and then taking care of yourself around it, the voice loses its purpose for
existence and fades away, at least till next time there is a difficult feeling you are
resisting!
Letting the voice time share in your body.

77
This is probably more likely to be helpful for someone who is not totally intimidated by the
voices and who feels they are not likely to get completely out of control. The way it works is
to just to set a time when you can experiment with having a particular voice have "control"
of your body, at a time when it is unlikely to cause any problem. (You should only attempt
this if you feel you could take back control should the voice attempt anything that will cause
trouble.) What is helpful about doing this is that you get to know the voice in a different
way, and may even find something positive about it. For example, you may find that an
angry voice has a very firm, strong way of acting in your body, and you may find you can
eventually borrow some of this strength when you need it in various situations in your life.
You may also eventually come to see the voice as more just a "side" of yourself, and less
threatening because less alien. Not taking voices literally
- This means considering the possibility that voices may not literally mean what they
say: instead, they may be speaking in metaphor, they may be speaking poetically.
So while the voice may insist for example that you "jump in the river" it might really
mean that you should get more into the flow of things, and not hold yourself back so
much. So, instead of just doing what the voice says, or just fighting with it because
you don't want to literally jump in the river, you could think about what the voice
might be really trying to say.
- Another way to not take the voices literally is to try out carrying out their demands
in your imagination, rather than literally. For example, if the voice wants you to cut
yourself, try imagining that you are cutting yourself, or that you already have done
so, and notice what changes, notice what the feelings are and what shifts inside you.
(This is very similar to the method above, where you focus on how it feels to be a
victim of the voice.)
Allowing your identity to be wider than you are in the habit of letting it be:
- Consider example of someone who wants to lose weight: they are sure who they are
is a person that entirely wants to lose weight, and is willing to give up desserts in
order to do so. Then they see a piece of chocolate cake, and suddenly, there is the
temptation to eat it. If the person is rigid about who they think they are, that they
are a person who doesn't want desserts, then they can only see the temptation to
eat the cake as coming from someone or something else, maybe a demon or an
unpleasant voice. The chocolate cake example is kind of silly, because usually people
are able to accept that there are two parts of themselves, one part that wants to diet
and another part that wants cake, so they can be wide enough in their identity to let
both parts in. But what about bigger conflicts?
- A person who wants to live may find it really difficult to accept an urge to kill
themselves. A person who wants to be conventional sexually may have a hard time
accepting urges to be gay or otherwise different sexually. A person who wants to be
peaceful may have a hard time with urges to kill or hurt others. These are very
serious conflicts. One way people can try to resolve them is to simply decide that
"the real me" only wants what is good or conventional, while the "evil" or "nasty"
ideas and impulses come from something else, like from voices.

78
- This solution could be called "making the self more narrow." Making the self more
narrow has its advantages, in that it can help a person feel that his or her own self is
good and peaceful. But the disadvantage is that the urges and temptations are still
alive somewhere, and they will live as voices and demons if not allowed to live as
parts of the self.
- Another way the self can get narrow: let's say the person identifies themselves as
kind of weak and incapable, for whatever reason. Something strong within them
might be seen as foreign, as not themselves. So maybe the person connects with the
strong part by thinking of it as an exterior spirit and feels helped by this. This can be
helpful, but since the strength is seen as exterior to the person, in time it can take its
own direction that may not be helpful to the person. For example, they might start
out noticing a "spirit" as helping in some strong way, but later the "spirit" wants to
take some direction that the person doesn't want to go. So "spirit helpers" can
easily become "demon opponents."
- Allowing yourself to be wider, means seeing the thing that seems to be either
opposing you or helping you as being part of the bigger you. In other words, you can
see yourself as wider, more complex than how you usually see yourself. You can be
wide enough to include things like urges to hurt yourself or others, urges to do
strange things, to be different sexually, or whatever. Being wider doesn't mean you
will necessarily let these urges take over, but it means allowing them to be part of
the mix that makes up you.
- Advantages to allowing yourself to be a wider person: You can talk about your
experience more the way most people do, which allows you to relate better to
conventional people. In other words, you can talk about how you are "beating
yourself up" instead of being attacked by a spirit, or how "part of me wants to kill
him" instead of "the voices are telling me to kill him" etc. By allowing yourself to be
wider, you are no longer as "pure" but you also don't have to feel as different from
"normal" people.
- This is not to say that the way "normal" people look at things is always the best way,
or always right. Maybe there are times when we would be better off identifying
ourselves in a narrow rather than a wide way. But if we have a choice about it at any
given time, we may be able to choose a way of looking at it that is most helpful to
ourselves at any given time.
Being kind to the voice
- Voices are often distressing, but it's easy to forget that they may be even more
distressed themselves. Treating them with kindness may really surprise them, and
result in some big changes! When you hear the distressing voice, take a step back
mentally, and imagine that it may really be troubled, and is causing trouble only
because it is desperate. You can take an attitude toward the voice similar to the

79
attitude a parent might take toward an injured, frightened, or tired child who is
being obnoxious.
- For example, a man may be bothered by a voice that calls him names and is very
threatening when he has to be around strangers. He may be planning to go the
store and knows this is likely to upset the voice. Instead of arguing or fighting with
the voice about his plans he could say to it: "I know that going to the store with all
the people around is really hard for you! Do you have any ideas about anything that
might help you feel safer while I do the shopping?" The voice might be helped by
something that is strictly imaginary, like imagining a tropical beach that the voice
can go to while the person is shopping. Or perhaps the voice would have a more
practical suggestion, like going to the store at a time when fewer people are around,
or having a better shopping list so the trip is less confusing.
- Notice in the above example, the person did not give in to the voice, but was kind to
it and considered its needs. This might not work right away (the voice may still be
distrustful and obnoxious) but eventually the relationship between the person and
the voice might change.
Getting better at telling the difference between "voices" and what actual people are
saying.
- Some people seem to always be able to tell when it is their "voices" talking and
when it is that they are listening to actual people, or the radio announcer, or
whatever. Other people have a harder time with this, and sometimes the voices
trick them into thinking that other people are saying things that they aren't. This can
cause lots of confusion and chaos! If this is a problem for you, here are some things
you can try:
- It might help to just pay attention and be on the lookout for this. Voices
trick people much more easily when they are being inattentive.
- Notice if there are certain things the voices really like to say. If you start
hearing people around you, or the radio announcer, saying these things, be
alert: it might really be the voices.
When what you are doing for coping isn't working:
- Try something different! Anything at all that you do differently might be just what
you need to be successful.
- You could even try something "completely different" or even the exact opposite of
what you were trying before.
Rediscovering your dreams and getting on with your life
While doing something just to distract yourself from the voices may have limited
usefulness, doing something because it connects with your dreams and because it makes

80
you feel fulfilled as a human being may be much more helpful! In other words, instead of
thinking you can't pursue your dreams because the voices cause too much trouble, try
finding right now some things you can do to take steps toward your dreams. Every time you
take some meaningful step, you win, and you prove that you and not the voices are in
control of your life!
Keep in mind that for this to work, you don't need to make the voices stop, you just
need to find ways to do what is most important to you whether the voices continue or not.
This focuses your attention on what you want to do, not on the voices.
What to do if you are trying to pay attention to some constructive activity but then
you notice you have started paying attention to the voices instead: just direct your
attention back to the constructive activity. Remember why you are doing it and why it is
important to you.
Other Types of Coping
- You may fine entirely different methods of coping as you pay attention to what
works for you: good luck in your experiments!
Basic Idea: that the origin of psychosis is in a retreat into the imagination, trying to make
imagination substitute for the extended world. This is fun at first but then the mind (or
imagination), in an attempt to re-engage the person with the extended world, quits
presenting positive images and presents images of danger, force, and hostility, attempting
to push the person into coping with what is unfriendly. The person, however, because he or
she is believing that the world of imagination is the extended world, finds him or herself
reacting to the imagined challenge as though it wore an actual challenge from the extended
world. Since the challenge is not "real" however it cannot be defeated, and so the person is
entirely stuck. One solution is for the person to notice that the imagined challenge can itself
be fought with the force of active imagination; doing so restores the neutrality of
imagination, leaving the person able to re-engage with the extended world.
Or, voices could start as a scared person tries to protect him or herself by imagining all
possible danger and anticipating it. The person goes from "this is ambiguous - it might be
that those people are talking about me" to actually "hearing" what it is feared they might be
saying. The person then reacts to what "might be" happening as though it really were
happening - classic panic. Similar only opposite causality on the grandiose side, where
person instead imagines what might really be great that is going on.
In the first model above, the voices begin as a kind of "addiction" or seduction, into which
the person buys into a positive feedback loop because of the appearance of a payoff. This
creates a dependence. The person then fears the absence of the voice and can be bullied by
the voice as a result, with the positive feedback then being the panic related to the
withdrawal. In the second model, it is panic that starts directly to create the feedback.
(Even then, we could say there is a hidden grandiosity or addiction, in that the person
imagines they cannot cope with losing whatever it is they are panicking that they are losing.)
Another way of looking at voices: as a dramatization of emotion. The brain may attempt to
dramatize an emotion that is being cut off or ignored (maybe because the person is already

81
overwhelmed). The problem gets worse as the person, or the persons around the person,
see the dramatization as "craziness" and cuts that off rather than see the sense, or the
emotion, within it.
Developing judgement about voices is key. If a "negative" voice, need to decide to what
extent it is helping one deal with a negative situation, and to what extent it is being too
extreme. The same is true of positive voices: to what extent are they helping and to what
extent are they getting one too carried away. This is really the same task as deciding when
emotions are helping and when they are going too far. Of course, when one is traumatized
the ability to judge what is too much, is overwhelmed.
Can think of voices as part of self, or think of all entities as part of one consciousness, think
of them as split off but really part of one mind.
Can just agree to disagree with voices, rather than get sucked into arguing. "Yes I know that
you think I'm worthless, it's ok with me if you think that, you have a right to your opinion. I
on the other hand see some value in what I am doing and in what I am capable of doing in
the future. I understand you don't agree. It's ok with me that you disagree with me."
When a negative voice speaks up, use that as a reminder to do some self-care for yourself.
Or use it as a reminder to do some constructive self-talk - say to yourself the things that a
friend or a good coach or a positive voice might say to you. Focus on that positive,
constructive message instead of what the negative voice has been saying.
Make an audiotape of the worst things voices might say. Play it over and over again until it
doesn't make you anxious anymore.
If unclear if voices are physically real (like hearing voices while alone at one's apartment,
that might be the neighbors) try making an audiotape & check it out.
Paying attention to how you set yourself up to be vulnerable to voices. For example,
thinking you have to live up to some standard of perfection, then whenever you don't you
are vulnerable to a voice that berates you for not doing it.
Focus on creating periods without being bothered by voices, rather than paying attention to
the voices. At first these might be short, later they could get longer. Pay attention to what
makes these periods happen, measure them, etc.
If you tell yourself you will have to stop the voices before you succeed, then you will pay lots
of attention to them as you try to figure out how to stop them (and less attention to the
world.) But if you actually pay more attention to the world, and less to the voices, then they
lose power. Sort of like bullies - often the best way to control them is to ignore them.
Make fun of voices as a method. First write out a script of what voices usually say. Then,
have a friend help you (it helps to make a tape of this you can listen to later.) Have the
friend say the statements on the script in his/her most silly voice possible. (They might try
to sound like a cartoon character, or say things in a very high pitched voice.) You repeat

82
back exactly what the "voice" said each time. Later you can listen to the tape as a reminder
that you don't have to take the voice seriously.
Making peace with the voices, "peace with justice." A bullies into buddies kind of thing.
Just as in meditation one identifies a thought by just thinking "thought" and then redirecting
ones attention, one could just identify "voice" and then redirect attention.
Voices - in addition to not taking them literally, can try not taking them "all the way." Voices
may represent parts of the brain that don't talk in shades or subtleties - they say then turn
right & go over cliff, but really mean turn right & act as if you were going over cliff, they
assume other parts will click in and get you to change course before you actually go over the
cliff. Like voices that ask for suicide - maybe really they just want you to kill something
about your current pattern of living.
Can have a person role play someone in their life who causes problems for them, to develop
a wider perspective on that person. Can use the same method, have the client role play a
voice, have it explain its perspective.
Making friends with voices - treat disagreements as temporary and consider attributions of
positive intent underneath surface hostility (either for self-protection by the part or to aid
the whole self in some way (at least an intent to do so.)
Something like eft - even though my voice is hyperactive, I accept myself and look forward
to a great future. Or even though I'm feeling very anxious about the voice, I accept my mind
just as it is in this moment. (NOTE how eft puts "acceptance and commitment" into one
sentence.
How voices are like poorly behaved children, feed off negative attention.
Being kind and open to reasonable influence, but also having firmness and boundaries (like
in good parenting or other relationships.)
Have people role play the voices, to find out more about it. Also to shift their sense of a
center, so they can sense that in some sense they have always been the voice. So their
sense of identity can "decenter" resulting in an expanded sense of self.
"love your enemy" is key with voices - or MPD - if you learn this, you can expand
your sense of identity, I'm not just my body I'm the world.
A person often jumps quickly to the perspective of another person looking at self, makes a
statement from that perspective, then jumps back to seeing the statement from the
perspective of self before becoming conscious of having done it. (dissociating having don it,
and/or the problem is just speed.) If a person actually takes that outside perspective for a
while, to own it, and own the process of saying things to self from that perspective, then it is
more likely to be seen as a habit that can be changed.

83
Becoming your own boss: how to invent a better boss that the voices that order you
around.
The do-over. Whatever a voice tells you, see what may have been of value in its expression.
For example, if it says you are stupid, it may be reminding you that there are important
things you don't know. In the do-over, tell yourself the same critical content in a more
adult, subtle, and balanced way, in your own words. As what you tell yourself becomes
more well-rounded and complete, you won't need the voice as much, will pay less attention
to it, and it will fade.
Getting people to reflect on where other people may be coming from, or an improved
"theory of mind" is a similar skill to seeing where a voice may be coming from, what
interests it may have
An over-emphasis on trying to control one's inner world leads to more confusion between
inner and external - because stuff one fails to control is what is seen as external. But getting
confused between internal and external worlds leads to inner confusion and distress,
leading often to greater attempts to control the inner world! This creates a vicious circle,
much like the circle created when people try too hard to get rid of anxiety.
Voice feeds on attention - so a voice that no one listens to isn't much. Can use Izzy Kalman's
"feed the pigeons" to make them go away as an example.
Negotiation - find interests under positions - voices may threaten torture but may be most
interested in attention - integration is the goal, like with MPD
How something healthy may be a center of something that initially seemed totally sick. Like
one of my clients working on recovery, a voice that once almost killed him in a horrible way,
is now part of his personality that helps him take on healthy challenges. Like in fairy tales,
you meet some strange character, have to fight at first to establish respect, then it can
become an ally
People block their feelings, become less aware of the sources of the feelings, feelings
become more problematic - then the mental health system makes it harder for people to
relate to such feelings by encouraging people to not even look for sources, "it's a
biochemical imbalance". Same goes for blocking a voice or a perspective.
A general method to get along with people with a different perspective “that’s so
interesting! …. that you experience it that way! Here’s how it is for me…. Someone attacks
you, you make a self-deprecating remark, this shows you can find some truth in their
perspective.
A good worksheet: look at what is for me to decide vs. what is for voice to decide, what is
for voices to decide for themselves. Like, it’s up to the voice to decide if it likes what I’m
doing, while it’s up to me to decide if I like it, it’s up to voice to decide if it would like me to
kill myself, but up to me to decide if I really want to or not.

84
Technique for deal with voices: take a 3
rd
position, I am not the voice or the one who hears
the voices, I am the one who has to understand and integrate both of them.
For a disturbing voice, either find or create a counter voice, that effectively contradicts the
disturbing voice. Then you can choose to either listen to the disturbing voice, the counter
voice, or to anything in between. You have a range of options.
Stress interpretation: see voices as a sign of too much stress, respond by taking it easy
rather than stress about the voices being present. (The voices are just an indicator of stress
not the cause, they are the smoke, not the fire. Though stressing about the voices can feed
the fire.)
Interpreting voices as something less extreme, or finding something less extreme to do to
honor the impulse behind the voice. This can work with more than just anger.
Can use a negative voice as a reminder to focus on one’s positive intention, as being like the
Zen master with a stick. Can thank it for its reminders.
Look around the room, name every object you see. This lowers anxiety and gets the more
“objective” part of your mind activated.
How starting and stopping voices can give you a sense of control. You can’t always be
controlling them but you know you have influence if you decide you need or want to.
If voices are just thoughts or imagining a monologue or dialogue, plus imagining what it
would sound like, then it figures that the less one cares about it or has an interest in it, the
less likely it would be to occur. But of course catastrophic thoughts about the meaning of
voices, or grandiose thoughts about the meaning of them, would lead to a greater interest
in imagining it further. (Part of the problem in psychosis is loss of distinction between
imagining what something might be, and seeing what it might be. When the thing is the
imagination itself, of course, there is no distinction.)
A “stress interpretation” of how to cope with voices – don’t concern oneself with the voice
at all directly. Instead, do two things. One, find a way not to stress about the existence of
the voice or what it is saying. Second, find a way to reduce the stress that probably
triggered the voice in the first place. (The voice itself can often be used as a clue to what
the stress was that triggered it. For example, if a person is viciously attacked by a person for
a particular failure, that suggests the person is stressing over that failure, and could work on
how to stress less about it, perhaps by understanding it better, making some changes, or
some focused self-forgiveness.)
People who hear an apparently destructive voice often over-rely on making themselves
smaller than the voice, which is what is involved in distraction, or trying to shut out the
voice. These methods involve focusing the person away from the voice, on an area of
consciousness that is smaller than the whole person, so that the voice is shut out. A
problem with this strategy is that it gives the person a smaller sense of themselves, since
they are training themselves to only identify with the part of them that doesn’t include the

85
voice. This can ultimately lead to a person feeling small and weak, while the voice, free to
move around in all of the person’s consciousness, can increasingly seem large and powerful.
No wonder people feel weak in comparison to it.
One alternative strategy is to deliberately focus on the voice, as an object of study.
So one can record exactly what it says, how often it says it, what identity it claims, ask it
questions, etc.
A person who can both focus away from the voice, and focus on the voice, can allow
themselves a broader focus as well, sensing themselves as a bigger human being who
includes the voice as just one part or aspect. This allows the person to feel bigger than the
voice, accepting its existence while being in no danger from it.
Stages of dealing with voices:
“Oh my God what is it!”
“I need to do anything so I don’t hear it (but I still do).
This is trying to make one’s focus smaller. Can work as a temporary measure to regroup and
get strength to face the voices, but is a poor permanent method, because it makes the
person feel smaller, and gives the voice more power.
“Fuck it I’m going to have a life anyway, so what if I hear a voice”
Person turns and faces the voice, expands focus to include the voice as just one aspect of a
much larger mind and life. If this is done sincerely, voice may fade away, or become just
part of overall self.
Same dynamics are involved in dealing with panic or other emotional problems. These
dynamics can be diagramed, with a large circle showing the whole self, with the initial “oh
my god” shown as focus on distress around the voice, then the avoidance stage shown as
focus on a small area away from the voice which makes the person seem small and voice
bigger, then the third stage shown as willingness to face any distress and see self as bigger
than the voice (maybe could use a stage of expanding focus to also include the voice while
keeping in mind the more peaceful resolved areas of self, rather than just focusing on
distress. How this applies to trauma too.
Trying to make a voice go away is like trying to make a critic go away, which is a variation of
trying to be CERTAIN. The person wants certainty beyond any doubt, and sees it as a
problem if doubt is being expressed anywhere, so the voice is seen as a huge problem. (The
setup for having a voice is that the person avoids thinking through their doubts, so that
these can easily self-organize into a voice.) It is actually accepting the voice and the doubt it
expresses that is likely to cause the voice to disorganize, as it loses its purpose. Since the
person accepts that doubt exists, there is no longer a sharp distinction between the
perspective of the voice and that of the person. If the voice continues, it is more likely to be
friendly.
Use of disarming method with voices. A key technique. This allows a way out of combat
with voices, and allows the person to work on integrating any positive intent or helpful

86
fragment from the voices while appropriately resisting any bad ideas. Avoids over-reactions
of any kind.
Talking to oneself in terms of “we” and “us” and “ourselves.” As in “Why are some of us
wanting to cut our wrists? How will we be better off if we do that?” This highlights the way
there is diversity but that we all hang together – could encourage teamwork. A downside if
it makes people have more trouble transitioning to using “I” when dealing with the external
world.

87
Coping with distressing voices or experiences
Step 1: Identify when and how the voices or distressing experience interferes with an identify value or
life goal
Describe voice or experience:
How/when does voice interfere?
How intense is your Distress with voices right now:
(0-10, with 10 being the most distressing)
Voices significantly interfere with my life when it is at a rating of: (0-10)
Step 2: Examine past coping and plan for future coping. Make a List
Helpful things I have done to deal with this experience
Unhelpful things I tried to deal with this experience
New ideas: look at list to identify new ideas for coping that will help me reach my valued goals
Adapted with permission From Yakoobian et al., 2007 CBT client manual.
88
Best Practices in Schizophrenia Treatment (BeST) Center
Cognitive Behavioral Therapy (CBT-p) Initiative
Selected Resources
List of Coping Strategies for Hallucinations
Distraction Focusing Meta-cognitive
Methods
Humming Correct the cognitive distortions in the voices Use schema focused
techniques
Talking to yourself Respond rationally to voice content Acceptance
Listen to modern music Sub vocalization Assertiveness
Listen to classical music Dismiss the voices Use a biological model
Prayer Remind yourself that no one else can hear
the voice
Consider shamanistic views
of voice hearing
Meditation Phone a voice buddy and tell them the voice
is active
Consider cultural aspects of
voice hearing
Use a mantra Remember to take antipsychotic medication Use positive logging to
refute negative beliefs
about the self
Painting Demonstrate controllability by bringing the
voices on
Use a continuum relating
your own worth to that of
other people
Imagery Give the voices a ten minute slot at a specific
time each day
List your positive
experiences in life
Walking in the fresh air Play a cognitive therapy tape discussing
voice control
List your achievements,
friendships etc.
Phone a friend Use a normalizing explanation Act against the voices
(show them that you are
better than they say)
Exercise
Use rational responses to reduce anger
Use a relaxation tape List the evidence in favor of the voice content
Yoga List the evidence against the voice content
Warm bath
Use guided imagery to practice coping with the
voices differently
Call your mental health
professional
Role play for and against the voices
89
Best Practices in Schizophrenia Treatment (BeST) Center
Cognitive Behavioral Therapy for Psychosis (CBT-p)
Selected Resources
List of 60 Coping Strategies for Hallucinations
Distraction Focusing Meta-cognitive
Methods
Attend the day center/
drop in
Remind yourself that voices are not actions
and need not be viewed that way
Watch TV Remind yourself that the voices don’t seem to
know much
Do a crossword or other
puzzle
Remind yourself that you don’t need to obey
the voices
Play a computer game Talk to someone you trust about the voice
content
Try a new hobby Use rational responses to reduce shame
Use rational responses to reduce anxiety
Use a diary to manage stress
Use a diary to manage your time
Plan your daily activities the night before
Use a voice diary in a scientific manner
Mindfulness
Try an earplug (right ear first if right handed)
90
Working with Negative
Symptoms

91
Daily Schedule
Day/Time Planned Activity Actual Activity How it Felt
Pleasant 0-10:
Productive o-10:
Pleasant 0-10:
Productive o-10:
Pleasant 0-10:
Productive o-10:
Pleasant 0-10:
Productive o-10:
Day/Time Planned Activity Actual Activity How it Felt
Pleasant 0-10:
Productive o-10:
Pleasant 0-10:
Productive o-10:
Pleasant 0-10:
Productive o-10:
Pleasant 0-10:
Productive o-10:
92
Negative Symptoms: A diminishment of normal functioning – something that has been taken away.
According to the DSM-5:
1.
Diminished emotional expression – “Reduction in the ability to express emotion in the face, eye
contact, intonation of speech and movements of the hand, head, and face that normally give an
emotional emphasis to speech.”
•
Appearing to lack emotion.
•
Decreased capacity for intimacy
•
A lack of warmth and thoughtfulness
2.
Avolition – “A decrease in motivated self-initiated purposeful activities.”
•
Loss of interest in everyday activities
•
Reduced ability to plan or carry out activities
•
Neglect of personal hygiene
•
Social withdrawal
•
Loss of motivation
•
Diminished ability to focus
•
Reduced pride in taking a sense of responsibility
•
Apparent lack of willingness to follow a treatment plan when ill
3.
Alogia – “Diminished speech output.”
4.
Anhedonia – “The decreased ability to experience pleasure from positive stimuli, or a
degradation in the recollection of pleasure previously experience.”
•
Activity monitoring diary can be particularly helpful.
•
Have the client rate their sense of pleasure or contentment before, during, and after the
activity they have chosen. Because they have a hard time remembering pleasure they
experienced during an activity, they have a difficult time anticipating pleasure, so it is
important to highlight their responses to pleasurable activities.
5.
Asociality – “An apparent lack of interest in social interactions and may be associated in
avolition, but it can also be a manifestation of limited opportunities for social interactions.”
•
Inability to read social signals such as body language
•
Social withdrawal
Negative symptoms are present with other psychotic disorders, but are particularly prominent with
schizophrenia. Diminished emotional expression and avolition tend to be the two negative symptoms
that are particularly noticeable with schizophrenia.
93
Positive symptoms: Behaviors not seen prior to the onset of the illness. These aspects of personality are
added as the illness progresses.
According to the DSM-5:
1.
Delusions - Fixed beliefs that are not based in reality.
•
Are not changed in light of contradictory evidence
•
Subtypes include:
• Persecutory – beliefs that one is going to be harmed is the most common
• Referential – beliefs that certain comments, gestures, or cues are directed
at oneself
• Grandiose – believing that one has exceptional abilities
• Erotomanic – falsely believing that someone is love with him/her
• Nihilistic – believing that a major catastrophe will occur
• Somatic – preoccupations regarding health and organ function
•
Bizarre – if they are not plausible and not understandable to same culture peers, and
are not part of normal experience (e.g., “there is a chip in my brain”, or “some of my
internal organs are not my own”).
•
Thought withdrawal – “Someone or something has taken away my thoughts”
•
Thought insertion – “Someone or something as inserted thoughts into my brain”
•
Delusions of control – “I’m being acted upon or manipulated by some outside
force”
•
Non bizarre – Beliefs that do not have convincing evidence, such as “I’m under
surveillance by the police or the FBI.”
2.
Hallucinations – “Perception like experiences that occur without external stimuli.”
•
Appear very real and have the impact of normal perceptions
•
Not under voluntary control
•
Can occur through any of the senses, but the most common is auditory
i.
Not perceived as one’s own thoughts
ii.
Usually perceived as voices that can be familiar or unfamiliar
3.
Disorganized thinking/speech – Difficulty speaking and organizing thoughts
•
May result in stopping speech in mid-sentence
•
Putting words together in meaningless ways (“word salad”)
4.
Disorganized motor behavior – May show in a number of ways
•
Childlike silliness
•
Unpredictable agitation
•
May be noted in any type of goal directed behavior which can disrupt ability to
perform activities of daily living (ADLs)
94
Working with Delusions

95
Delusions Level 1
Delusions Level 2
Engagement
•
Make talking about beliefs safe
•
Find time and place that is safe
Gain understanding
•
What are client’s beliefs
•
Help client explore the many ways –
unassuming questions that explore how
client’s beliefs affect him/her
•
Don’t confront delusions
Improve daily living
•
Focus on reachable goals
•
Work on stress reduction and emotion
regulation
o
Relaxation
o
Activities tied to personal interests and
values
•
Try to improve sleep
Neutral, Curious stance
•
Suspend disbelief
•
Ask questions to help you understand – again,
unassuming questions
•
Small checks for flexibility of thinking
Re-focus on another activity, topic, goal if needed.
All of Level 1
Formal Assessments; Consider
•
PSYRATS
Explore using peripheral, unassuming questions
•
How does that work?
•
I’m curious…etc.
•
Ask eye-witness type questions
o
Who, what, when, where…
Consider impact of trauma
Develop a formulation
•
On what evidence are they basing thoughts
•
Given past history/experience, discover how
current beliefs make sense
o
Work with self esteem
•
Are they experiencing an unusual sensations?
o
Help them make sense of that
•
What cognitive errors might they be making
•
What behaviors keep the behavior going
Lower distress and improve coping
•
Stress reduction
•
Improve sleep
Belief modification - meta-cognitive methods
•
Alternate beliefs activity
•
Pie Chart activity
•
De-centering
•
Cost/benefit analysis of dwelling on a concern
of belief
•
Identify ways to check out new belief systems
o
Behavioral experiments
o
Reality testing

96
CBT-p methods for working with delusions (paranoia)
Engagement: Alliance building strategies such as conversations about neutral topics and look for
areas that client feels confident to tell you about (hobbies, interests, etc.)
Exploratory questions (peripheral and Socratic)- to gain understanding and help client to explore
belief objectively; explore clients’ goals and purpose and check to see if delusion causes
DISTRESS or INTERFERENCE with goals and purpose (this is key)
May use self-monitoring forms to organize experiences (thought, mood, physio record)
Formulation: Key information to be identified and reviewed with client (Freeman & Garety, 2006)
o
On what evidence are they basing their thoughts? Teach them how to explore how they
are making sense of their experience and to check evidence
o
Thinking about the person’s life and past experience, how do current concerns make
sense? Were they bullied or abused in their life? Would make sense that they would
expect others to be threatening.
Self-esteem concerns often underlie paranoid and suspicious beliefs. One target
may be to find ways to improve self-esteem in other aspects of their life
o
Is person responding to confusing or puzzling experience (e.g., physiological, odd
sensory experience). It is not uncommon for individuals to interpret unusual sensory
experiences (e.g., depersonalization; detachment; dizziness) as threatening or imposed.
Normalize and help client to develop alternative explanations for the experience.
o
How is the person reasoning about their experience (jumping to conclusions, leaving out
information, tendency to blame others for coincidental or chance events, or other
thinking error?). The most common reasoning error in paranoia is jumping to
conclusions (40-70%). Other key areas are over-estimating risk and assigning blame for

97
chance events. Educate clients re commonness of these thinking habits and practice
identifying this type of thinking in other aspects of their life.
o
What behaviors keep the thoughts going? Anxiety and worry; sleep loss? Avoidance or
other safety behaviors? Help client to modify these areas
When the person is well, what type of behaviors do they engage in?
Action phase: Lower stress and improve coping (in order to be more functional, less isolating)
o
Stress and anxiety reduction strategies
o
Improve sleep
Action phase: Belief modification:
o
Identify what it would mean for the client if the belief changed. What would be
better/worse?
o
Introduce idea of continuum (rather than all or nothing, maybe a scale of 0 – 100)
o
Generate alternative perspectives/explanations for experiences (can be organized with
pie chart, or other tool). Need to proceed carefully when considering alternative
explanations.
o
Identify ways to check beliefs and test new explanations or (Behavioral experiments/
Reality checks). Will need to help client make clear predictions and carefully evaluate
their predictions based on evidence, including how the client will interpret evidence that
supports and/or refutes their current belief.
o
Find ways to support new beliefs if they are more functional for the client
Freeman, D. & Garety, P. (2006). Helping patients with paranoid and suspicious thoughts: A cognitive-
behavioral approach. Advances in Psychiatric Treatment, 12, 404-415.
98
Special Topics

99
Suicide
•
50% suffer from comorbid substance use disorder
•
50% suffer from comorbid depression
•
10% suffer from comorbid anxiety disorder
•
Childhood adversity (ACEs) can be a causative factor in onset of
schizophrenia
•
Odds of suicide attempts are 6xs higher among those with schizophrenia
when compared with those w/o SZ; up to 15% commit suicide
•
Substance use and depression resulted in higher rates of suicide attempts
•
A comorbid anxiety disorder resulted in 70% less likely to attempt suicide
(better problem solving, communication, better skills to negotiate the world
•
Highest risk post discharge and in the first 90 days

100
Homicide
•
Those who commit a homicide are more likely to have delusional beliefs at the
time of the event
•
Delusional beliefs have been reported in 33-95% of murderers with MMD
•
This has more to do with the fear for his/her own life that is provoked by
the delusion – it is generally not about an intent to harm out of anger or
revenge
•
More likely to be committed when intoxicated at the time of the event
•
Important to pay attention to patients who are fatigued, in despair, delusional,
depressed, particularly when there is a lot of stress happening in client’s life
occurring
•
Ask about
•
Depression, delusion, chronic stress
•
Thoughts of killing children (in women with schizophrenia)
•
Specific perceived perpetrators (in men with schizophrenia)

101
Crisis Planning
Among the treatment team and other caregivers,
including family:
•
Decide how the plan will be triggered – What will that first person do?
•
Have a contact list ready (names and phone numbers) – therapists, case
managers, physicians, nurses
•
Put together an emergency crisis card that includes the list of contacts
•
Decide if a power of attorney needs to be identified
•
Decide what will trigger a 911 call
Adherence

103
Adherence factors:
IM
PORTANCE
Generally, how important is it for you to take your medication(s) on a scale from 1 (not important) to 10
(very important)?
Why did you place yourself at that particular point on the scale?
W
hat would have to change for it to become more important for you to take your medication?
C
ONFIDENCE
Generally, how confident are you that you will take your medication as prescribed on a scale from 1(not
confident) to 10 (very confident)?
Why did you place yourself at that particular point on the scale?
W
hat would have to change for you to become more confident in taking your medication?
104
SATISFACTION
Generally, how satisfied are you with your medication on a scale from 1(not satisfied) to 10
(very satisfied)?
Why did you place yourself at that particular point on the scale?
What would have to change or be different for you to be more satisfied about your medication?

105
ADHERENCE SOLUTIONS CARD
Include dose and time of day that the medication is taken
T
hings I need to talk to my doctor about at my next appointment:
Record strategies that will help me to remember to take medication
(e.g., reminders- keep medication next to the coffee pot to remember
to take morning medication) in the box below:
R
eview the things that help me with taking medication (e.g., “the
benefits of medication are…”) and record them in box below:
Record ways that I can reward myself for taking medication and steps to
goals:
Box 1
Box 2: I would like the medicine to help me with:
So that I can reach my goal of:
Box 3
Box 4
Box 5

106
My Name: ___________________________________
I am at my best when I am doing the following:
________________________________________________________________________
_
_______________________________________________________________________
________________________________________________________________________
My Values and Goals:
Values: The most important things in my life are…
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
___________________________________________________________________
Goals For Recovery: I would like medicine to help with these goals
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
___________________________________________________________________
Inspired by: Deegan, P., Carpenter-Strong, E., Drake, R., Naslund, J., Luciano, A., Hutchinson, S. (2017). Enhancing clients’
communication regarding goals for using psychiatric medications. Psychiatric Services in Advance. doi: 10.1176/
appi.ps.201600418
107
Outcome Measures
BAVQ – R
108
CHADWICK, PAUL, LEES, SUSAN, BIRCHWOOD, MAX
The revised Beliefs About Voices Questionnaire (BAVQ-R)
(from The British Journal of Psychiatry 2000 177: 229-232)
There are many people who hear voices. It would help us to find out how you are
feeling about your voices by completing this questionnaire. Please read each
statement and tick the box which best describes the way you have been feeling in
the past week.
If you hear more than one voice, please complete the form for the voice which is dominant.
Thank you for your help.
Name: .....................................................
Age: .....................................................
Disagree
Unsure
Slightly
Agree
Strongly
Agree
1
My voice is punishing me for
something
I have done
2
My voice wants to help me
3
My voice is very powerful
4
My voice is persecuting me for no good
reason
5
My voice wants to protect me
6
My voice seems to know everything
about me
7
My voice is evil
8
My voice is helping to keep me sane
9
My voice makes me do things I really
don’t want to do
10
My voice wants to harm me
11
My voice is helping me to develop my
special powers or abilities
12
I cannot control my voices
13
My voice wants me to do bad things
14
My voice is helping me to achieve my
goal in life

109
15
My voice will harm or kill me if I
disobey or resist it
Disagree
Unsure
Slightly
Agree
Strongly
Agree
16
My voice is trying to corrupt or destroy
me
17
I am grateful for my voice
18
My voice rules my life
19
My voice reassures me
20
My voice frightens me
21
My voice makes me happy
22
My voice makes me feel down
23
My voice makes me feel angry
24
My voice makes me feel calm
25
My voice makes me feel anxious
26
My voice makes me feel confident
When I hear my voice, usually ...
Disagree
Unsure
Slightly
Agree
Strongly
Agree
27
I tell it to leave me alone
28
I try and take my mind off it
29
I try and stop it
30
I do things to prevent it talking
31
I am reluctant to obey it
32
I listen to it because I want to
33
I
willingly follow what my voice tells
me to do
34
I have done things to start to get in
contact with my voice
35
I seek the advice of my voice
Psychotic Symptom Rating Scale (PSYRATS)
110
PSYCHOTIC SYMPTOM RATING SCALES
A Auditory hallucinations
1 Frequency
0
Voices not present or present less than once a week
1
Voices occur for at least once a week
2
Voices occur at least once a day
3
Voices occur at least once an hour
4
Voices occur continuously or almost continuously i.e. stop for only a few seconds or minutes
2
Duration
0
Voices not present
1
Voices last for a few seconds, fleeting voices
2
Voices last for several minutes
3
Voices last for at least one hour
4
Voices last for hours at a time
3
Location
0
No voices present
1
Voices sound like they are inside head only
2
Voices outside the head, but close to ears or head. Voices inside the head may also be present
3
Voices sound like they are inside or close to ears and outside head away from ears
4
Voices sound like they are from outside the head only
4 Loudness
0
Voices not present
1
Quieter than own voice, whispers
2
About same loudness as own voice
3
Louder than own voice
4
Extremely loud, shouting
5
Beliefs regarding origin of voices
0
Voices not present
1
Believes voices to be solely internally generated and related to self
2
Holds < 50% conviction that voices originate from external causes
3
Holds ≥ 50% conviction (but < 100%) that voices originate from external causes
4
Believes voices are solely due to external causes (100% conviction)
6
Amount of negative content of voices
0
No unpleasant content
1
Occasional unpleasant content (<10%)
2
Minority of voice content is unpleasant or negative (<50%)
3
Majority of voice content is unpleasant or negative (≥ 50%)
4
All of voice content is unpleasant or negative
Psychotic Symptom Rating Scale (PSYRATS)
111
7
Degree of negative content
0
Not unpleasant or negative
1
Some degree of negative content, but not personal comments relating to self or family e.g.
swear words or comments not directed to self, e.g. ‘the milkman’s ugly’
2
Personal verbal abuse, comments on behavior e.g. ‘shouldn’t do that or say that
3
Personal verbal abuse relating to self-concept e.g. ‘you’re lazy, ugly, mad, perverted
4
Personal threats to self-e.g. threats to harm self or family, extreme instructions or commands to
harm self or others
8
Amount of distress
0
Voices not distressing at all
1
Voices occasionally distressing, majority not distressing (<10%)
2
Minority of voices distressing (<50%)
3
Majority of voices distressing, minority not distressing (≥50%)
4
Voices always distressing
9
Intensity of distress
0
Voices not distressing at all
1
Voices slightly distressing
2
Voices are distressing to a moderate degree
3
Voices are very distressing, although subject could feel worse
4
Voices are extremely distressing, feel the worst he/she could possibly fee
10
Disruption to life caused by voices
0
No disruption to life, able to maintain social and family relationships (if present)
1
Voices causes minimal amount of disruption to life e.g. interferes with concentration although
able to maintain daytime activity and social and family relationships and be able to maintain
independent living without support
2
Voices cause moderate amount of disruption to life causing some disturbance to daytime
activity and/or family or social activities. The patient is not in hospital although may live in
supported accommodation or receive additional help with daily living skills
3
Voices cause severe disruption to life so that hospitalization is usually necessary. The patient is
able to maintain some daily activities, self-care and relationships while in hospital. The patient
may also be in supported accommodation but experiencing severe disruption of life in terms of
activities, daily living skills and/or relationships
4
Voices cause complete disruption of daily life re9uiring hospitali6ation. 8he patient is unable to
maintain any daily activities and social relationships. Self-care is also severely disrupted.
11
Controllability of voices
0
subjec5t believes they can have control over the voices and can always bring on or dismiss them
at will
1
Subject believes they can have some control over the voices on the majority of occasions
2
Subject believes they can have some control over their voices approximately half of the time
3
Subject believes they can have some control over their voices but only occasionally. The
majority of the time the subject experiences voices which are uncontrollable
4
Subject has no control over when the voices occur and cannot dismiss or bring them on at all
Psychotic Symptom Rating Scale (PSYRATS)
112
B Delusions
1
Amount of preoccupation with delusions
0
No delusions, or delusions which the subject thinks about less than once a week.
1
Subject thinks about beliefs at least once a week
2
Subject thinks about beliefs at least once a day
3
Subject thinks about beliefs at least once an hour
4
Subject thinks about delusions continuously or almost continuously
2
Duration of preoccupation with delusions
0
No delusions
1
Thoughts about beliefs that last for a few seconds, fleeting thoughts
2
Thoughts about delusions last for several minutes
3
Thoughts about delusions last for at least 1 hour
4
Thoughts about delusions usually last for hours at a time
3 Conviction
0
No conviction
1
Very little conviction in reality of beliefs, < 10%
2
Some doubts relating to conviction in beliefs, between 10-49%
3
Conviction in belief is very strong, between 50-99%
4
Conviction is 100%
5
Distress
0
No distress
1
Beliefs cause slight distress
2
Beliefs cause moderate distress
3
Beliefs cause marked distress
4
Beliefs cause extreme distress, could not be worse
6
Disruption to life caused by beliefs
0
No disruption to life, able to maintain independent living with no problem in daily living skills.
Able to maintain social and family relationships (if present)
1
Beliefs cause minimal amount of disruption to life, e.g. interferes with concentration although
able to maintain daytime activity and social and family relationships and be able to maintain
independent living without support
2
Beliefs cause moderate amount of disruption to life causing some disturbance to daytime
activity and/or family or social activities. The patient is not in hospital although may life in
supported accommodation or receive additional help with daily living skills
3
Beliefs cause severe disruption to life so that hospitalization is usually necessary. The patient is
able to maintain some daily activities, self-care and relationships while in hospital. The patient
may be also be in supported accommodation= but experiencing severe disruption of life in
terms of activities, daily living skills and/or relationships
4
Beliefs cause complete disruption of daily life requiring hospitalization. The patient is unable to
maintain any daily activities and social relationships. Self-care is also severely disrupted.

113
Name: ......................................................
RAS-DS (Recovery Assessment Scale – Domains and Stages)
Instructions: Below is a list of statements that describe how people sometimes feel about themselves and
their lives. Please read each one carefully and circle the number to the right that best describes you at the
moment. Circle only one number for each statement and do not skip any items.
DOING THINGS I VALUE
UNTRUE
A bit
TRUE
Mostly
TRUE
Completely
TRUE
1
It is important to have fun
1
2
3
4
2
It is important to have healthy habits
1
2
3
4
3
I do things that are meaningful to me
1
2
3
4
4
I continue to have new interests
1
2
3
4
5
I do things that are valuable and helpful to others
1
2
3
4
6
I do things that give me a feeling of great pleasure
1
2
3
4
LOOKING FORWARD
UNTRUE
A bit
TRUE
Mostly
TRUE
Completely
TRUE
7
I can handle it if I get unwell again
1
2
3
4
8
I can help myself become better
1
2
3
4
9
I have the desire to succeed
1
2
3
4
10
I have goals in life that I want to reach
1
2
3
4
11
I believe that I can reach my current personal goals
1
2
3
4
12
I can handle what happens in my life
1
2
3
4
13
I like myself
1
2
3
4
14
I have a purpose in life
1
2
3
4
15
If people really knew me they would like me
1
2
3
4
16
If I keep trying, I will continue to get better
1
2
3
4
17
I have an idea of who I want to become
1
2
3
4
18
Something good will eventually happen
1
2
3
4
19
I am the person most responsible for my own improvement
1
2
3
4
20
I am hopeful about my own future
1
2
3
4
21
I know when to ask for help
1
2
3
4
Recovery Assessment Scale – Domains and Stages (RAS-DS – Research Version 3).
©2015 Nicola Hancock and The University of Sydney.
Not to be copied or used for any other purpose without written permission from the author
(nicola.hancock@sydney.edu.au)

114
LOOKING FORWARD (continued)
UNTRUE
A bit
TRUE
Mostly
TRUE
Completely
TRUE
22
I ask for help, when I need it
1
2
3
4
23
I know what helps me get better
1
2
3
4
24
I can learn from my mistakes
1
2
3
4
MASTERING MY ILLNESS
UNTRUE
A bit
TRUE
Mostly
TRUE
Completely
TRUE
25
I can identify the early warning signs of becoming unwell
1
2
3
4
26
I have my own plan for how to stay or become well
1
2
3
4
27
There are things that I can do that help me deal with
unwanted symptoms
1 2 3 4
28
I know that there are mental health services that help me
1
2
3
4
29
Although my symptoms may get worse, I know I can handle it
1
2
3
4
30
My symptoms interfere less and less with my life
1
2
3
4
31
My symptoms seem to be a problem for shorter periods of
time each time they occur
1 2 3 4
CONNECTING AND BELONGING
UNTRUE
A bit
TRUE
Mostly
TRUE
Completely
TRUE
32
I have people that I can count on
1
2
3
4
33
Even when I don’t believe in myself, other people do
1
2
3
4
34
It is important to have a variety of friends
1
2
3
4
35
I have friends who have also experienced mental illness
1
2
3
4
36
I have friends without mental illness
1
2
3
4
37
I have friends that can depend on me
1
2
3
4
38
I feel OK about my family situation
1
2
3
4
Recovery Assessment Scale – Domains and Stages (RAS-DS – Research Version 3).
©2015 Nicola Hancock and The University of Sydney.
Not to be copied or used for any other purpose without written permission from the author
(nicola.hancock@sydney.edu.au)

115
THE RECOVERY ASSESSMENT SCALE – DOMAINS AND STAGES (RAS-DS)
•
Untrue • Mostly true
•
A bit true • Completely true
•
Doing Things I value
– Personal, not societal values
•
Looking Forward
–
Viewing self outside context of illness
–
Hopeful for the future
•
Mastering My Illness
–
Focus on control and management of symptoms, not amelioration of
symptoms
•
Connecting and Belonging
–
Greater diversity in social relationships
–
Family and broader communities
–
Reciprocated and personally satisfying
38 items with Likert scale with 4 rating categories from:
Four recovery domains
You can use one section at a time, or all sections at the same time. It’s up to you
and wheat you believe your client needs.
Find the free manual and workbook online at https://ras-ds.net.au/
“Or type in RAS-DS My mental health recovery measure” in your browser to get complete
instructions and workbook for use with clients
Nicola Hancock et al., 2014 If you choose to use the RAS-DS, please email Nicola at:
nicola.hancock@sydney.edu.au. She will automatically send you updates as they are created.

116
Name: Rating interval: B, 3, 6, 9, 12 Date:
DIALOG
Totally
Dissatisfied
Very
Dissatisfied
Fairly
Dissatisfied
In the
middle
Fairly
Satisfied
Very
Satisfied
Totally
Satisfied
Additional help
Wanted? Yes/no
How satisfied are you with your
Mental health?
How satisfied are you with your
Physical health?
How satisfied are you with your
Job situation?
How satisfied are you with your
Accommodations/housing
How satisfied are you with your
Leisure activities?
How satisfied are you with your
Partner/family?
How satisfied are you with your
Friendships?
How satisfied are you with your
Personal safety?
How satisfied are you with your
Medication?
How satisfied are you with your
Practical help you receive?
How satisfied are you with your
Meetings with mental health
professionals?
Pick the top three things that you would like to work on: Updates since last review/Progress to Goals
1
2
3
DIALOG was developed by Stephan Priebe <[email protected]k . Used with permission

117
DIALOG STRATEGY
•
Area client really wants to work on
•
Satisfaction rating below 4
•
Distress associated with mental health item
•
Always helpful to purposefully review areas of progress and decline
•
Always helpful to purposefully review areas of progress and decline
1.
Understanding (Socialize and Target)
2.
Looking forward (Action phase)
3.
Exploring options (Action phase)
4.
Agreeing on actions (Review and Take Home)
Priebe, et al (2007; 2012)
Introduce DIALOG as a way to help you work together
Re-administer every 2-3 months
Select no more than 3 domains to work on at a time
Guidelines to select a focus
For review sessions
DIALOG “4-step” approach applied to target areas:
118
Study Guides

119
One-Pager Summary Notes for Session 1
Section 1: Introduction
What is CBT-p and what are some “versions” of this approach?
Why should we use a team-based model for working with psychosis?
Section 2: Empathy exercise
What is it like for someone who experiences psychosis?
Section 3: On being human
What did I learn about how my brain works?
Section 4: Understanding Schizophrenia
Important notes to help me understand Schizophrenia
Section 5: Ways to think about Schizophrenia
Of the three ways of thinking about schizophrenia, which ones most inform my view?
Most inform my agency’s view of treatment?
Stigma
Biology
Recovery
Finish
What do I want to learn more about?
What is one learning step I will take after this course? When will I do it?

120
Series # 1.2 (Day 1 section 2)
Take home work
Review of Take-home work – What did you find most interesting or surprising as you
reviewed the different websites provided in our series schedule? And what about it was
interesting to you?
Strategies informed by CBT-p
Define engagement:
Define normalization:
What is the “Adaptive Mode”:
How do you find common ground with the clients you work with?
A Plan for Goals
All of the choices below are a pathway to creating a goal, but what is the most effective
pathway to finding a goal for you and your client to work on?
a. Brainstorming, Values, strengths, obstacles, choosing the best goal, stepping
stones, review, revise
b. Goals, values, obstacles, brainstorming, choosing the best goal, stepping stones,
review, revise
c. Choosing the best goal, obstacles, values, review, stepping stones, brainstorming,
revise
What activity might you do if your client is having a difficult time identifying their values?
Acceptance and Empathy – tough but important question
When we talk about “acceptance,” are we saying that the client really has to accept
his/her diagnosis? Are we saying that they have to agree with their diagnosis? If we are
not saying that, then what is it we want our clients to accept?

121
How might you search for empathy from yourself when you can’t fully relate to what the
client is going through?
Is it ok to take a break from the session and come back 5 minutes later, or to walk around
the agency with your client to help soothe the client’s distress? What other techniques
might you use to help your client feel safer in the office or in your car (or wherever).
Normalization and Education
You’ve told your client that what they are experiencing is a continuum of what is “normal”
across our US population. What evidence can you use to support your position with the
client?
Stress and Schizophrenia
What are some stressors that might result in psychosis experiences?
How can the “Stress Bucket” help explain to your client how they might change how they
manage their stress?
Name two ways the Stress Bucket can be used to provide the client with tools to navigate
stress in their life?

122
Study Guide for Day 1 Session 3 (1.3)
Take-Home Work
What did you learn about yourself from completing the Stress Bucket activity?
START Model
Define all of the components of the START model and give a brief example of how you might
approach each of these components
S:
T:
A:
R:
T:
CBTp Model:
On the CBTp Triangle shown below, briefly describe what each corner represents and what is
represented by the middle space in the triangle:

123
Interview Techniques:
What are three questions you might ask in order to translate the CBTp model into a full
understanding of the experience (not to be confused with the 3Cs technique):
1.
2.
3.
Write out the Three Question Technique (The 3 Cs):
1.
2.
3.
Cognitive Restructuring is something only a licensed therapist can use with a client. Case Managers
should not attempt to use this technique:
True:
Explain:
False:
Explain:
Emotion Regulation
A higher level of distress is experienced when which technique is used to manage thoughts (circle all
that apply):
Avoidance Acceptance Re-appraisal
Suppression Rumination Vocalizing the emotion
What is one extremely important activity is necessary to do with your client when they return with a
completed mood monitoring survey (this is not a trick question):
Name three methods for self-soothing:
1.
2.
3.
List three common phrases you could use with your client when you notice he/she is distressed
1.
2.
3.
Describe what a “formulation” and how it is used:
Take-Home Work: Look at the case of Joe, put it into the cognitive model, and respond to the
questions on the back of the page.

124
Study Guide for Day 2 Session 1 (2.1)
Take-Home Work
How did the formulation go? What did you learn?
START Model
Write down a statement you might make during each phase of the START Model
S:
T:
A:
R:
T:
CBTp Model:
Using the diagram below, outline how you might describe the CBTp Model. Why would we do this?
Components of CBTp Therapy
Write out the 8 main components of CBTp therapy
1.
2.
3.
4.
5.
6.
7.
8.

125
Describe anosognosia as if you were describing it to a family member of a client you are working
with.
What do you think of training the client to become a good “CBTp client,” and why.
What is Socratic Dialogue and Guided discovery? How might you use it in therapy with a client you
are working with now?
How might you use a formulation with your client?
Complete a formulation on a client you are working with (no identifying information please) to share
with the class.

126
Study Guide for Day 2 Session 2 (2.2)
Take-Home Work
How did the mini-formulation go? What did you learn?
Working with thoughts
How do you guide the client when working with a thought record?
Think of a game that you can play in the office that might help the client learn the 3Cs and describe
below (e.g. I play waste-basketball by catching the thought (written on a piece of paper and then
balled up, discover a new thought that is more reality oriented, and throwing the old thought away –
basketball style)
What does “flexible thinking” mean?
All this looks easy. Looks like the same things case managers are taught to do. What makes it
different in the “therapy world?”
What do you think of training the client to become a good “CBTp client,” and why.

127
What is Socratic Dialogue and Guided discovery? How might you use it in therapy with a client you
are working with now?
How might you use a formulation with your client?
Complete a formulation on a client you are working with (no identifying information please) to share
with the class.

128
Study Guide for Day 2 Session 3 (2.3)
Take-Home Work
Were you able to list techniques to use for thoughts, emotions, behavior? Any Questions?
Voices
List 5 insights you gained in yourself when you participated in the voice hearing activity
Using your own experience to help with your client’s experiences.
Based on your experience of the voice hearing activity, how will you practice differently as a result of
your insights.
What is the most important thing about using a voice diary?
How will you use the voice diary to collaborate with your client?
List 10 things that might cause voice hearing, other than a diagnosis of schizophrenia or psychosis.
It is very likely that the voices individuals hear are reflective of ?

129
Is it possible that voices are thoughts the client hears?
In what way might trauma play a role in voice hearing?
Is it really possible that the client is actually hearing something? How do we know?
What are 5 incredibly important questions to ask an individual who is experiencing distressing voices.
If we can’t help the client get rid of the voices, what would be the next target to focus on?
Delusions
Name 3 techniques to use when a client is experiencing delusions.
How hard will it be for you to drop a reality based “seed thought”?
How hard will it be for you to focus on improving daily living rather than helping the client to
eliminate the voices?
Homework: Look for a place in your practice to use a voice diary and explain it to your client. Ask if
they would be willing to use a voice diary. Make plans to review the voice diary the next time the
client returns.

130
Study Guide for Day 2 Session 4 (2.4)
Take-Home Work
1.
What did you learn from the Delusion Behavioral Experiment?
2.
In what ways could this experiment have been set up more effectively?
There are 5 aspects of negative symptoms that need to be considered when preparing to
intervene. What are those 5 aspects?
1.
2.
3.
4.
5.
Would it be fair to say that someone who is presenting with negative symptoms is unmotivated
and really has no interest in changing their behavior? Why?
What safety maintenance behavior is a part of negative symptoms? Describe how that
maintenance behavior works?
What is a “hierarchy of activities?”
What are the main points you would review when teaching a client about Behavioral Activation.
OK, so now you have a fairly well completed Activity Monitoring worksheet? What do you do with
it?
What do you look for?

131
What is the goal of Behavior Activation?
Name the three ways to address common barriers when using Behavior Activation?
You’ve got a patient with severe negative symptoms who also has psychosis. What issue do you
attend to most at the beginning of treatment? Why?
Describe what to say when a client indicates that in no way does he/she want to take medication?
Describe what to say when a client indicates that he/she might take medication, he/she is
undecided.
What if a client indicates that he/she is willing to take meds, but is often so forgetful, the meds get
forgotten most of the time.

132
Study Guide for Day 3 Session 1 (3.1)
Take-Home Work
What new skills have you been using? What is your experience in using these new techniques?
What do we mean when we refer to “acculturational stage” ?
What coping skills are similar across cultures?
How might other cultures differ from our western culture in terms of relationships, boundaries,
environment, and who holds power?
What might be different for other cultures in terms of help-seeking by the client and/or family?
In what areas do you personally need to work on to reduce biases you may have about working
with other cultures (we all have biases that need to be worked on – everyone of us!)

133
Name five reasons we even bother to use outcome measures
1.
2.
3.
4.
5.
Given your scope of practice (your employment role), which outcome measure that we talked
about in this session might you consider using on a client on your case load? Why?
Why do families need to be invited, as much as possible, in the treatment of psychosis?
What techniques might you discuss with family members to help them negotiate effective
communication with their loved one who suffers from psychosis?
Is it possible for an entire family to engage in maintenance behaviors (safety behaviors) that keep
them from understanding what their loved one is going through? What might those behaviors look
like?
If you have ever been a victim of stigma, can you describe what feelings and thoughts you had at
the time? (no need to describe the situation, only the feelings and thoughts you had at the time).

134
Name: Agency: Title of your role: Date:
Study Guide 3.2 YES Undecided NO
I commit to learning the CBTp model, formulation, and
practice skills.
☐ ☐ ☐
I commit to discussing these skills during supervision,
and I will discuss how they can be used effectively with
clients.
☐ ☐ ☐
I understand that should I submit a recording for
fidelity rating, that the rating I receive is not reflective
of my value and worth as a therapist/provider (neither
positive or negative). I will keep in mind that the
fidelity rating is only for my own improvement as a
CBTp informed therapist/provider.
☐ ☐ ☐
I’d like to submit fidelity recordings and learn how to
work toward fidelity of CBTp skills as measured by my
supervisor (if supervisor is trained in CBTp) or by CBTp
staff at NEOMED (Harry Sivec, PhD/Valerie Kreider,
PhD, LPCCS).
☐ ☐ ☐
Should an inter-agency learning collaborative form
(e.g. CBTp trained providers from other NEOMED
partner agencies), I would like to be a part of that
group for my own learning purposes.
☐ ☐ ☐
Thank you for taking the time and energy to be with us during this training. We feel grateful
to have so many therapists from around Ohio interested in being available for this vulnerable,
and workable, population.
We invite you to hang with us (the NEOMED CBTp faculty/staff) and continue to learn,
discover, and collaborate on ways that CBTp informed practice can answer the hopes and
dreams of those who suffer from psychosis and schizophrenia.

Practicum For Therapists
Practice session 1: The First Session
Each dyad should practice a separate portion of the session.
1. The first dyad practices the S and T of START: getting to know your client and what they
want to work on.
2. The second couple practices engagement and empathy. This would be the A part of the
START model, and while we don’t normally think of engagement and empathy as
“active/action” items or interventions, sometimes it’s the only action we can give
depending on the severity of current psychosis symptoms. Think about using techniques
such as normalizing, guided discovery (to get a better understanding of the presenting
problem), psychoeducation…etc.
3. The third dyad practices setting an agenda (we will pretend here that setting the agenda
took the whole session so completing the RT of START to identify the agenda for further
sessions
Role play: client who has paranoia and/or negative symptoms
Skills to practice:
1. Engagement and empathy (10 minutes)
2. Setting an agenda (10 minutes)
3. Use the START Model throughout the session with each dyad doing their respective
portion of the START model.
Main focus is to use the adaptive mode and empathy to get through setting an agenda (DO NOT
PROBLEM SOLVE)
• Find interests and find adaptive mode (Desired practice outcome)
• Find interests/strengths and most important issues to discuss today. If more than one issue is
defined, identify an agenda in order of importance of issues to address this session.
• Help person translate interest into value-based goal if time permits
Experience of the Therapist using a CBTp strategy
Experience of the Client in this session. Give the therapist feedback.

Practicum For Therapists
Take 5 minutes after each 10 min session to give and get feedback from peers in
your group. Discuss what it was like to be the client and the therapist

Practicum For Therapists
Feedback for Practicum 1
S Socialize, support, safety (mindset for beginning each visit): Make it comfortable. Be kind and
friendly. Refrain from advice giving.
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
T Target: Identify target to work on and/or review during the meeting. The target is usually
related to the client’s goals.
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
A Action: Apply one intervention/technique relevant to the client’s goal within the work specific
to your role. Define the therapeutic framework that supports each of these activities.
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
R Review: Check the client’s understanding of your discussion and ask for feedback about the
meeting.
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
T Take home-work: Identify things to work on before the next meeting. Send the client home
with necessary material, including a business card with the next scheduled meeting.
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
Practicum For Therapists
Practice session 2: Working with Thoughts and Emotions
Switch roles every 20 minutes. Your group will need to get through an entire session in one hour, with
each dyad picking up where the previous dyad left off. So this is the REAL A (Action or intervention)
session.
Role play a client who has very critical voices
1. Identify unhelpful/ineffective thinking patterns (10 mins)
2. Skills to practice: Continue on from the previous session, but change therapists and clients.
Keeping the issue the client wants to talk about in mind, collaborate with client to choose one of
the following to work on with your client (15 mins).
Each dyad can continue on with the intervention decided upon in the previous dyadic session,
or, the dyad may try to practice a different intervention just to play around and get some
practice.
1. Thought Record for Belief (Alternative Thinking/Cognitive restructuring)
2. The 3Cs
3. Decision Balance (and cons
4. CBT Triangle
5. List of Unhelpful Thinking Habits
3. Debrief: Discuss the session and collaborate on homework. Discuss what the client understands
about the topic of discussion. Make sure they understand the homework assignment. Anything
we could do differently next time? (10 mins)
Therapist: Anything further they might want to investigate, ask about before next session.
Debrief:
Experience of the Therapist using a CBTp strategy
Experience of the Client in this session. Give the therapist feedback.

Practicum For Therapists
Take 5 minutes after each 10 min session to give and get feedback from peers in
your group. Discuss what it was like to be the client and the therapist
Feedback for Practicum Session 2
S Socialize, support, safety (mindset for beginning each visit): Make it comfortable. Be kind and
friendly. Refrain from advice giving.
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
T Target: Identify target to work on and/or review during the meeting. The target is usually
related to the client’s goals.
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
A Action: Apply one intervention/technique relevant to the client’s goal within the work specific
to your role. Define the therapeutic framework that supports each of these activities.
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
R Review: Check the client’s understanding of your discussion and ask for feedback about the
meeting.
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
T Take home-work: Identify things to work on before the next meeting. Send the client home
with necessary material, including a business card with the next scheduled meeting.
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________

Practicum For Therapists
Practice session 3: Working with Voices and Delusions
Role play a client who: has voices and/or paranoia; Switch roles every 20 minutes
Skills to practice: Learning to feel comfortable working with voices and delusions
Desired outcome: Client to arrive at a different perspective on the voices
1. Understanding the voices (15 mins)
o Ask permission to talk about the voices (required)
o Asking directly about the voices (who, age, male/female, content, how many, etc.)
o What emotions does client experience
o What has the client tried already to reduce the voices
o When are the voices at their worse; when are they better
o What does client do when they hear the voices
o Do others hear the voices
2. Discover what the client believes about his/her voices (15 mins)
o What did I tell myself when it happens?
o What would I tell a friend if they had this experience; or what might they tell me in this
situation?
o Are voices all powerful or is there room for negotiation with them?
o Do they intend harm to client or someone they love, or are they helpful?
o Are the voices accurate?
o What if what the voice is saying is not accurate or just wrong?
3. Choose a coping skill to get to understand and work with the voices, assign homework, and
have client summarize what he/she learned and what was helpful (15 mins)
o Cognitive restructuring
o Voice Diary
o Evidence for and against negative content of voices
o Behavioral coping methods for coping with voices
o Mindfulness and compassion activities
Experience of the Therapist using a CBTp strategy
Experience of the Client in this session. Give the therapist feedback.

Practicum For Therapists
Take 5 minutes after each 10 min session to give and get feedback from peers in
your group. Discuss what it was like to be the client and the therapist
Feedback for Practicum 3
S Socialize, support, safety (mindset for beginning each visit): Make it comfortable. Be kind and
friendly. Refrain from advice giving.
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
T Target: Identify target to work on and/or review during the meeting. The target is usually
related to the client’s goals.
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
A Action: Apply one intervention/technique relevant to the client’s goal within the work specific
to your role. Define the therapeutic framework that supports each of these activities.
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
R Review: Check the client’s understanding of your discussion and ask for feedback about the
meeting.
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
T Take home-work: Identify things to work on before the next meeting. Send the client home
with necessary material, including a business card with the next scheduled meeting.
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________

Practicum For Therapists
Case scenarios
For practicum, it is best to role play a client in a way that feels genuine. You can role play a client that
you know well who experiences certain symptoms to make it more authentic. Please do not make the
role plays too difficult as we are all here for a learning experience. If the provider is having a hard time,
the client should be a little easier to work with. If the provider is doing very well and session is going
very easily, consider making the client a little more difficult. If you do not have any examples that
would work for the role play, you can use the cases below as a starting point and then modify as
needed. Feel free to elaborate symptoms or to add areas of interest and hobbies to make the role play
realistic.
Paranoia:
Client is a young adult with religious based paranoia. Believes that bad things happen because of past
behaviors. Believes the devil is punishing him/her, especially when social interactions do not go well.
Tends to misperceive social cues. Whenever anything out of the ordinary happens, believes it is due to
the devil or demons. He / She stays at home most of the day playing video games and sleeping. Avoids
other people because negative feedback confirms belief that he/she will not be able to have a
relationship. Difficulty with concentration and short-term memory, makes it hard to process
conversations at times. Enjoys music, watching sports, strong faith beliefs, work is very important.
For acute paranoia: person believes they are being followed by a gang. Has made several calls to the
police and to family members. Wears a hat and jacket with effort to cover his face when out in public.
Appears tense and hypervigilant, looking around the room and “on alert”.
Negative symptoms:
Person is middle-aged, lives by self and has very few social connections. Stays home most of the time
and does not feel like doing anything. Children have moved away and has some regrets about their
childhood and blames self. Will Spend time on the phone with her child and these phone calls can last
for hours at a time. Sometimes, he/she loses sleeps and becomes more paranoid and holds the idea that
her child was abducted in the past. Does not feel like he/she can do anything, despite the fact that
he/she makes it to appointments regularly. Moves slowly, mostly due to age, but does get around.
Doesn’t think people will like him/her. The person has an interest in preparing food, especially desserts
and enjoys watching birds.
Voice hearing:
Person is middle-aged with a long history of hearing more than one voice. He/she will respond to
internal stimulation in public and then minimize that he/she is responding to voices. The voices are
insulting at times, calling him/her names and telling him/her not to shower or not to sleep in the
bedroom. Voice sometimes interfere with sleeping at night and with taking showers. Appearance is
somewhat dirty and disheveled. Person is sociable, likes music, movies, pets, and still helps elderly
parents at times.

141
Feedback for Practicum 3
S
Socialize, support, safety (mindset for beginning each visit): Make it comfortable. Be kind and friendly.
Refrain from advice giving.
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
T Target: Identify target to work on and/or review during the meeting. The target is usually related to the
client’s goals.
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
A Action: Apply one intervention/ technique or other action relevant to the client’s goal within the work
specific to your role. Define the therapeutic framework that supports each of these activities.
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
R Review: Check the client’s understanding of your discussion and ask for feedback about the meeting.
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
T Take home work: Identify things to work on before the next meeting. Send the client home with
necessary material, including a business card with the next scheduled meeting.
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
