
1
A Report
to the Nation
February 2001

Some 2 million American workers are victims of workplace violence each year.

Violence in the workplace. Every few days, there is another story on the news. One day, it may be a convenience store shooting;
the next, a sexual assault in a company parking lot; a few days later, it’s a disgruntled employee holding workers hostage,
or a student attacking a teacher.
Not surprisingly, the incidents of workplace violence that make the news are only the tip of the iceberg. What its victims all have in
common is that they were at work, going about the business of earning a living, but something about their workplace environment—
often something foreseeable and preventable—exposed them to attack by a customer, a co-worker, an acquaintance, or even a
complete stranger.
Some 2 million American workers are victims of workplace violence each year. It is estimated that costs of workplace violence to
employers is in the billions of dollars. Unfortunately, research into the prevention of violence in the workplace is still in its infancy.
In April 2000, The University of Iowa Injury Prevention Research Center took an important first step to meet this need by sponsoring
the Workplace Violence Intervention Research Workshop in Washington, DC. The goal of this workshop was to examine issues related
to violence in the workplace and to develop recommended research strategies to address this public health problem. The workshop
brought together 37 invited participants representing diverse constituencies within industry, organized labor, municipal, state, and
federal governments, and academia. The following is a summary of the problem of workplace violence and the recommendations
identified by participants at the workshop.
Solid information on what works, and what doesn’t, is urgently needed.

4
of customer/client incidents occur in the health care industry,
in settings such as nursing homes or psychiatric facilities; the
victims are often patient caregivers. Police officers, prison staff,
flight attendants, and teachers are some other examples of
workers who may be exposed to this kind of workplace violence.
Worker-on-Worker (Type III): The perpetrator is an employee or
past employee of the business who attacks or threatens another
employee(s) or past employee(s) in the workplace. Worker-on-
worker fatalities account for approximately 7% of all workplace
violence homicides.
Personal Relationship (Type IV): The perpetrator usually does
not have a relationship with the business but has a personal
relationship with the intended victim. This category includes
victims of domestic violence assaulted or threatened while
at work.
These categories can be very helpful in the design of strategies to
prevent workplace violence, since each type of violence requires a
different approach for prevention, and some workplaces may be at
higher risk for certain types of violence.
How often does workplace violence occur? An essential problem
with efforts to reduce workplace violence is that data are scattered
and sketchy, making it very difficult to study what works and what
doesn’t work to reduce violence in the workplace. The best data
available cover fatal events. There is less information available
concerning injuries from non-fatal events, economic impact on
businesses affected, lost productivity and other costs. Various
data collection systems have different ways of defining “at work,”
especially when there are ambiguities such as commuting and
. . . homicide remains the third leading cause of fatal occupational injuries for all
workers and the second leading cause of fatal occupational injuries for women
The Extent of the Problem
Workplace violence is receiving increased attention thanks to a
growing awareness of the toll that violence takes on workers and
workplaces. Despite existing research, there remain significant
gaps in our knowledge of its causes and potential solutions.
Even the extent of violence in the workplace and the number of
victims are not well understood.
In 1999, the Bureau of Labor Statistics recorded 645 homicides in
workplaces in the United States. Although this figure represents a
decline from a high of 1,080 in 1994, homicide remains the third
leading cause of fatal occupational injuries for all workers and the
second leading cause of fatal occupational injuries for women.
The number of non-fatal assaults is less clear. The National Crime
Victimization Survey, a weighted annual survey of 46,000
households, estimates that an additional 2 million people are
victims of non-fatal injuries due to violence while they are at work.
Addressing this problem is complicated, because workplace
violence has many sources. To better understand its causes and
possible solutions, researchers have divided workplace violence
into four categories. Most incidents fall into one of these categories:
Criminal Intent (Type I): The perpetrator has no legitimate
relationship to the business or its employees, and is usually
committing a crime in conjunction with the violence. These crimes
can include robbery, shoplifting, and trespassing. The vast
majority of workplace homicides (85%) fall into this category.
Customer/Client (Type II): The perpetrator has a legitimate
relationship with the business and becomes violent while being
served by the business. This category includes customers, clients,
patients, students, inmates, and any other group for which the
business provides services. It is believed that a large proportion
Type I: Criminal Intent
n May 2000, two men entered a Wendy’s in Flushing, NY, with the intent to rob the fast-food
restaurant. They left with $2,400 in cash after shooting seven employees. Five of the employees died and two
others were seriously injured.
This is an extreme example of Type I workplace violence: violence committed during a robbery or similar crime in the
workplace. Type I is the most common source of worker homicide. Eighty-five percent of all workplace homicides fall into
this category. Although the shootings in Flushing drew a great deal of media attention, the vast majority of these
incidents barely make the news. Convenience store clerks, taxi drivers, security guards, and proprietors of “mom-and-
pop” stores are all examples of the kinds of workers who are at higher risk for Type I workplace violence.
In Type I incidents:
• The perpetrator does not have any legitimate business relationship with the establishment;
• The primary motive is usually theft;
• A deadly weapon is often involved, increasing the risk of fatal injury;
• Workers who exchange cash with customers as part of the job, work late night hours, and/or work alone are at
greatest risk.
5
travel, volunteers or students in a workplace, or workplaces that
are also residences, such as farms or home offices. Sources of
information such as police, physician, workers’ compensation, or
employee reports may capture only one element—the violent
incident, or the injury, or the lost work time, or the setting (at
work)—but not the whole picture of the trauma resulting from
violence in the workplace. Finally, many non-fatal incidents,
especially threats, simply go unreported, in part because there is
no coordinated data-collection system to process this information.
Prevention
There are three general approaches to preventing workplace
violence:
• Environmental: adjusting lighting, entrances and exits, security
hardware, and other engineering controls to discourage
would-be assailants;
• Organizational/Administrative: developing programs, policies,
and work practices aimed at maintaining a safe working
environment;
• Behavioral/Interpersonal: training staff to anticipate, recognize
and respond to conflict and potential violence in the workplace.
There has not been adequate research, however, into the
effectiveness of these approaches for all types (I-IV) of workplace
violence. For example, most research to date on criminal intent
(Type I) violence in retail settings has focused only on environmen-
tal approaches. Although there have been some promising initial
findings, more research is needed to help businesses properly
protect their employees. Very little research has been conducted
on behavioral/interpersonal or organizational/administrative
approaches to prevention.
The Occupational Safety and Health Administration (OSHA) has
developed voluntary guidelines for the prevention of workplace
violence, including guidelines for specific industries such as late-
night retail, health care and social service, and community
workers. However, the effectiveness of these recommendations
has yet to be fully evaluated. Funding is urgently needed to
evaluate these guidelines.
The most troubling problem with existing research is that very
little of it has been conducted using rigorous scientific methods.
One of the papers prepared for this workshop (Peek-Asa, Runyan,
and Zwerling; see “Resources” on page 13 for more information)
describes a comprehensive review of research to date. The authors
raised a variety of concerns with a large proportion of the
research, including sample sizes that were too small, a lack of
appropriate control groups, publication without peer review, and
other problems. This lack of good research severely hampers
efforts to address the problem of violence in the workplace.
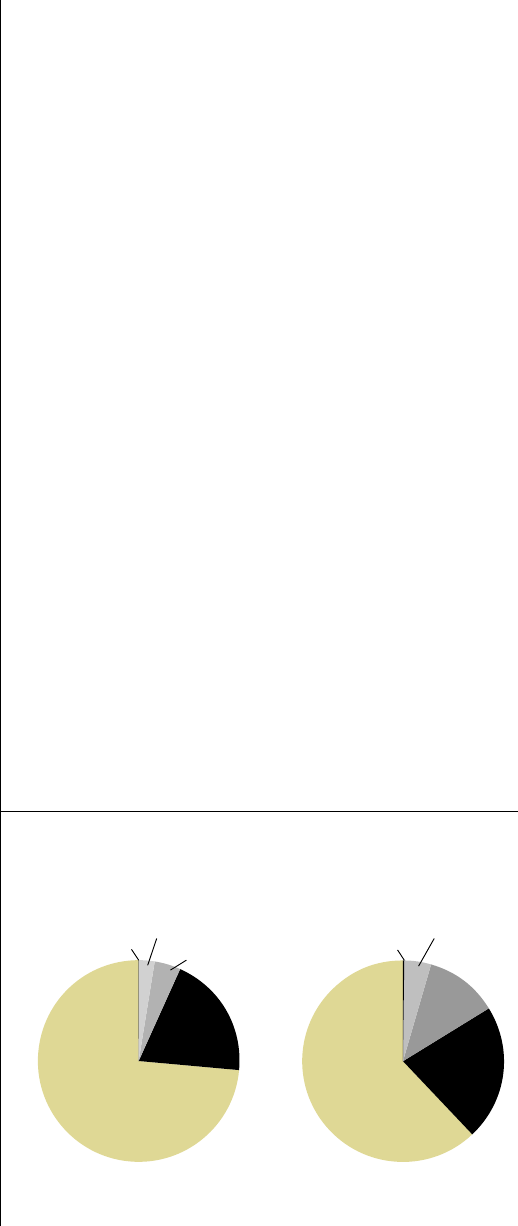
Rape and sexual assault 4.3%
Homicide 0.2%
Robbery
11.7%
Aggravated
assault
21.7%
Simple assault
62%
Rape and sexual assault 2.5%
Homicide 0.05% Robbery
4.2%
Aggravated
assault
19.7%
Simple assault
73.6%
Victims of Violence, 1992-96
Victimization in the Workplace All Victimizations
Source: National Crime Victimization Study, July 1998
6

Type II: Customer/Client
honda Bedow, a nurse who works in a state-
operated psychiatric facility in Buffalo, NY, was
attacked by an angry patient who had a history of
threatening behavior, particularly against female
staff. He slammed Bedow’s head down onto a counter after
learning that he had missed the chance to go outside with
a group of other patients. Bedow suffered a concussion,
a bilaterally dislocated jaw, an eye injury, and permanent
scarring on her face from the assault. She still suffers from
short-term memory problems resulting from the attack.
When she returned to work after recuperating, the
perpetrator was still on her ward, and resumed his threats
against her.
In Type II incidents, the perpetrator is generally a customer
or client who becomes violent during the course of a
normal transaction. Service providers, including health
care workers, schoolteachers, social workers, and bus and
train operators, are among the most common targets of
Type II violence. Attacks from “unwilling” clients, such as
prison inmates on guards or crime suspects on police
officers, are also included in this category.
In Type II incidents:
• The perpetrator is a “customer” or a client of the worker;
• The violent act generally occurs in conjunction with the
worker’s normal duties;
• The risk of violence to some workers in this category
(e.g., mental health workers, police) may be constant,
even routine.
7

8
Industry
Some employers have responded to the problem of workplace
violence by implementing measures to reduce the risk to their
employees. Different industries have different kinds of risks
depending on a multitude of factors, including the type of
business, populations served, management, employees, location
of the workplace, layout of the work area, and the relationship of
that business with the community.
Employers have attempted to increase safety by various means,
including:
• Physical security enhancements, such as lighting and cash
handling procedures, that make it more difficult to carry out a
violent assault (All Types);
• Threat management procedures, such as a team-oriented plan of
action in the case of a violent incident (All Types);
• Employee Assistance Programs (EAPs), to provide intervention
for at-risk employees (Type III and IV);
• “Zero tolerance” policies related to threatening or harassing
behavior (Type III);
• Employee training, to promote recognition of hazards and
appropriate responses to incidents of violence (All Types);
• Screening, to identify potentially high-risk employees (Type III);
• Company policies and training to facilitate employee comfort in
reporting threatening behaviors (All Types) and timely manage-
ment response to the employee reports;
• Hiring of security firms that specialize in prevention of
workplace violence (All Types).
In workplaces that have only infrequent incidents of violence,
many employers find it difficult to decide which safety measures
are most appropriate. This is especially true when faced with very
expensive or labor-intensive interventions. Private security
services and consultants abound, but there is limited scientific
information on which strategies work best for the various types of
There is no national legislation nor are there any federal regulations specifically
addressing the prevention of workplace violence.
Laws and Regulations
Federal: There is no national legislation nor are there any federal
regulations specifically addressing the prevention of workplace
violence. OSHA has published voluntary guidelines for workers in
late-night retail, health care, and taxicab businesses, but employ-
ers are not legally obligated to follow these guidelines.
State: To date, several states have passed legislation or enacted
regulations aimed at reducing workplace violence in specific
industries. California and Washington have enacted regulations
aimed at reducing patient-employee (Type II) violence in health
care settings. At least three states (Florida, Virginia, and Washing-
ton) have laws or regulations intended to prevent robbery-related
homicides (Type I) in late-night retail establishments such as
convenience stores. The Florida law is the most comprehensive.
Many convenience stores in Florida have found it easier to simply
close for business during the late-night hours (11 p.m. to 5 a.m.)
rather than make the changes required by the law. Neither the
legal changes nor the store closings have been evaluated as
strategies to prevent workplace violence.
State OSHA regulations: The states of California and Washington
both enforce regulations requiring comprehensive safety programs
in all workplaces, including the prevention of “reasonably
foreseeable” assault on employees.
Local: Taxi drivers appear to have by far the highest risk of fatal
assault of any occupation. Safety ordinances, such as those
requiring bullet-proof barriers in taxicabs, have appeared in
several U.S. cities, including Los Angeles, Chicago, New York City,
Baltimore, Boston, Albany (NY), and Oakland (CA). More study is
needed to assess these approaches.

Type III: Worker-on-Worker
ype III violence occurs when an employee assaults or attacks his or her co-workers. In some cases,
these incidents can take place after a series of increasingly hostile behaviors from the perpetrator.
Worker-on-worker assault is often the first type of workplace violence that comes to mind for many people,
possibly because some of these incidents receive intensive media coverage, leading the public to assume that most
workplace violence falls into this category. For example, the phrase “going postal,” referring to the scenario of a postal
worker attacking co-workers, is sometimes used to describe Type III workplace violence. However, the U.S. Postal Service
is no more likely than any other industry to be affected by this type of violence.
Type III violence accounts for about 7% of all workplace homicides. There do not appear to be any kinds of
occupations or industries that are more or less prone to Type III violence. Because some of these incidents appear to be
motivated by disputes, managers and others who supervise workers may be at greater risk of being victimized.
In Type III incidents:
• The perpetrator is an employee or former employee;
• The motivating factor is often one or a series of interpersonal or work-related disputes.
9

10
characteristics, say its critics, is not an effective predictor of
potentially violent behavior and may raise discrimination issues.
In general, labor unions favor an increase in voluntary implemen-
tation of workplace violence intervention by employers, coupled
with some mandatory provisions such as state legislation or a
mandatory OSHA standard. Labor also recognizes the need for
more research to determine which current OSHA guidelines and
other types of interventions are most effective in preventing
violent incidents in the workplace.
Recommended Workplace Violence Research Agenda
Workshop participants identified specific areas of research
needed for each of the four types of workplace violence. Interven-
tion research questions that need to be addressed include:
Criminal Intent (Type I):
• What are people doing now?
What factors predict employers’ choices of strategies to
prevent workplace violence?
How can employers choose appropriate workplace violence
prevention consultants?
Are current training programs effective?
• How effective are the OSHA guidelines?
• How many businesses are voluntarily complying with
OSHA guidelines?
• Do industry-specific environmental, organizational/administrative,
and behavioral/interpersonal control strategies work?
Client/Customer on Employee (Type II):
• How do staffing and the organization of work affect violence in
the health care setting?
• How effective are the OSHA guidelines?
workplace violence. In addition, businesses are often reluctant
to make their security methods public, not wanting to alarm
customers or tip off potential perpetrators, which makes it difficult
to evaluate those methods.
Employers are often in a difficult position when it comes to
responding appropriately to the problem of workplace violence.
They must avoid over-reacting, under-reacting, or reacting in a way
that exacerbates the problem. In addition, businesses may face
serious legal implications with some security measures. For
example, some kinds of pre-employment screening may be viewed
as discriminatory, but an employer could also face a “negligent
hiring” lawsuit if an applicant with a past history of violence is hired.
Labor
In the past decade, representatives of organized labor have
pushed for the recognition of workplace violence as an
occupational hazard, not just a criminal justice issue. Of particular
concern is the high rate of violent incidents targeting health care
workers (Type II violence). On some psychiatric units, for example,
assault rates on staff are greater than 100 cases per 100 workers
per year. Unions representing workers in the health care industry
suspect that “short-staffing” may play a role in this problem, but
there is little research into this issue to date.
Organized labor professionals or representatives have also
expressed concerns about workplace violence interventions that
target employee behavior, such as “zero tolerance” policies and
“worker profiling” designed to identify employees or potential
employees at risk for violent behavior. There is concern that zero
tolerance policies may be unevenly enforced and that they fail to
address some of the root causes of violence, such as stress or
situations leading to conflict. Profiling based on personal
. . . representatives of organized labor have pushed for the recognition of workplace violence as an
occupational hazard, not just a criminal justice issue.

11
Type IV: Personal Relationship
amela Henry, an employee of Protocall, an
answering service in San Antonio, had decided in the
summer of 1997 to move out of the area. The abusive
behavior of her ex-boyfriend, Charles Lee White,
had spilled over from her home to her workplace, where he
appeared one day in July and assaulted her. She obtained
and then withdrew a protective order against White, citing
her plans to leave the county. On October 17, 1997, White
again appeared at Protocall. This time he opened fire with
a rifle, killing Henry and another female employee before
killing himself.
Because of the insidious nature of domestic violence, it is
given a category all its own in the typology of workplace
violence. Victims are overwhelmingly, but not exclusively,
female. The effects of domestic violence on the workplace are
many. They can appear as high absenteeism and low
productivity on the part of a worker who is enduring abuse or
threats, or the sudden, prolonged absence of an employee
fleeing abuse. Occasionally, the abuser—who usually has no
working relationship to the victim’s employer—will appear at
the workplace to engage in hostile behavior.
In some cases, a domestic violence situation can arise
between individuals in the same workplace. These situations
can have a substantial effect on the workplace even if one of
the parties leaves or is fired.
Type IV violence:
• Is the spillover of domestic violence into the workplace;
• Generally refers to perpetrators who are not employees or
former employees of the affected workplace;
• Targets women significantly more often than men,
although both male and female co-workers and supervisors
are often affected.

12
. . . our understanding of workplace violence is still in its infancy. Much remains to be done
in the area of research, particularly in data collection and in intervention.
• How extensive is voluntary compliance with OSHA guidelines in
the health care industry?
• Do industry-specific environmental, organizational/administra-
tive, and behavioral/interpersonal control strategies work?
Worker-on-Worker (Type III):
• What is the relationship between corporate culture, the
organization of the workplace, security, and worker-on-worker
violence?
• How can public health data on threats and violence be improved?
• Are “zero tolerance” policies and profiling effective?
Personal Relationships (Type IV):
• How big is the problem? What is the impact of domestic violence
on the workplace?
• What strategies have been used by labor and management to
address this problem? How effective have they been?
• What is the legal situation? What duties do employers have
under state laws? Are there legal barriers to early interventions?
• Can businesses play a critical role in changing social norms
regarding domestic violence?
Conclusion
Workplace violence affects us all. Its burden is borne not only by
victims of violence, but by their co-workers, their families, their
employers, and by every worker at risk of violent assault—in other
words, virtually all of us. Although we know that each year
workplace violence results in hundreds of deaths, more than 2
million injuries, and billions of dollars in costs, our understanding
of workplace violence is still in its infancy. Much remains to be
done in the area of research, particularly in data collection and in
intervention. Without basic information on who is most affected
and which prevention measures are effective in what settings,
we can expect only limited success in addressing this problem.
The first steps have been taken. With the help of a broad coalition,
a number of key issues have been identified for future research.
However, research funding focused on a much broader under-
standing of the scope and impact of workplace violence is urgently
needed to reduce the human and financial burden of this signifi-
cant public health problem.
0 50,000 100,000 150,000 200,000 250,000 300,000
Retail sales
Teaching
Medical
Mental health
Transportation
Private security
Law enforcement
0%
20%
40%
60%
80%
100%
Type I:
Criminal intent
Type II:
Customer/Client
Type III:
Co/Past Worker
Type IV:
Personal relationship
85
3
7
5
Average Annual Number of Violent Non-Fatal
Victimizations in the Workplace, 1992-96
By Selected Occupations
Source: National Crime Victimization Study, July 1998
Total number of homicides=860 Source: Census of Fatal Occupational Injuries, BLS
Percent of Work-Related Homicides by Type, United States, 1997

13
Acknowledgements
This workshop would not have been successful without the
support of several agencies and individuals. We would like to
thank the National Institute for Occupational Safety and Health
(NIOSH) and the National Center for Injury Prevention and
Control (NCIPC) for the generous financial support that made the
workshop possible. We received valuable advice throughout the
process by the workshop’s planning committee: Ann Brockhaus
from Organization Resources Counselors; Lynn Jenkins from
NIOSH; Keith Lessner from the Alliance of American Insurers;
Corrine Peek-Asa from the Southern California Injury Prevention
Research Center; and Robyn Robbins of the United Food and
Commercial Workers International Union. The unique mix of
participants invited to the workshop is a credit to the planning
committee’s efforts. The review paper authors are to be
commended for their hard work spent preparing, presenting, and
revising their papers. While many persons too numerous to list
contributed to this workshop, we would like to single a few out for
special recognition. Injury Prevention Research Center Director
Craig Zwerling provided leadership throughout the process.
Associate Editor Leslie Loveless spent countless hours writing and
editing the reports and papers resulting from this workshop.
Carrie Kiser-Wacker from the UI’s Center for Conferences and
Institutes ensured that the workshop ran smoothly. And finally,
we would like to thank Carol Runyan for her closing summary at
the workshop and for writing the response paper.
We hope that the papers and recommendations from this workshop
will be the catalyst for a national initiative on workplace violence
intervention research. We appreciate the opportunity to organize
the workshop, which has produced this report to the nation.
James A. Merchant, MD, Dr PH, Dean and Professor
College of Public Health
Director, Public Policy Core
John A. Lundell, MA
Deputy Director
The University of Iowa Injury Prevention Research Center
Workshop Co-Directors
Resources
Five review papers, each addressing a specific aspect of workplace
violence, were prepared in conjunction with the workshop.
They appear in the February 2001 issue of the American Journal
of Preventive Medicine, at www.elsevier.com/locate/ajpmonline.
The papers are:
Barish RC. Legislation and Regulations Addressing Workplace
Violence in the U. S. and British Columbia.
Peek-Asa C, Runyan CW, Zwerling C. The Role of Surveillance and
Evaluation Research in the Reduction of Violence Against Workers.
Rosen J. A Labor Perspective of Workplace Violence Prevention:
Identifying Research Needs.
Runyan CW. Moving Forward with Research on the Prevention of
Violence Against Workers.
Wilkinson CW. Violence Prevention At Work: A Business
Perspective.
Up-to-date information and statistics on workplace violence are
available at the following web sites:
The OSHA web site on workplace violence, which includes
recommendations for prevention at http://www.osha.gov
The Bureau of Labor Statistics web site: http://stats.bls.gov
National Institute for Occupational Safety and Health:
http://www.cdc.gov/niosh
National Center for Injury Prevention and Control:
http://www.cdc.gov/ncipc
American Federation of State, County and Municipal Employees:
http://www.afscme.org/health/faq-viol.htm
California OSHA web site on Workplace Security:
http://www.dir.ca.gov/DOSH/dosh_publications/index.html

14
Participants
David Alexander
George Meany Center for Labor
Studies
Silver Spring, Maryland
Ileana Arias, PhD
Division of Violence Prevention
National Center for Injury
Prevention and Control
Centers for Disease Control and
Prevention
Atlanta, Georgia
Michael Arrighi
The Steele Foundation
Richmond, Virginia
Robert Barish
CAL/OSHA
San Francisco, California
Michele Beauchamp
OSH Compliance and Regulatory
Development
HRDC Labour Program
Ottawa, Ontario
Patricia Biles
U.S. Department of Labor/OSHA
Washington, DC
Bill Borwegen
Service Employees International
Union
Washington, D.C.
Ann Brockhaus, MPH
Organization Resources
Counselors, Inc.
Washington, DC
Joanne Colucci
American Express Company
New York, New York
Detis T. Duhart, PhD
Bureau of Justice Statistics
Department of Justice
Washington, DC
Raymond B. Flannery, Jr., PhD
Massachusetts Department of
Mental Health
Boston, Massachusetts
Lynn Jenkins, MA
Division of Safety Research
National Institute for Occupa-
tional Safety and Health
Centers for Disease Control and
Prevention
Morgantown, West Virginia
Spurgeon Kennedy
Office of Development and
Communication
National Institute of Justice
Washington, DC
Theodore Krey
The International Association of
Chiefs of Police
Alexandria, Virginia
Keith Lessner
Alliance of American Insurers
Downers Grove, Illinois
Jane Lipscomb, PhD
University of Maryland
School of Nursing
Baltimore, Maryland
Leslie Loveless, MPH
UI Injury Prevention
Research Center
Iowa City, Iowa
John A. Lundell, MA
UI Injury Prevention
Research Center
Iowa City, Iowa
Captain Jim McDonnell
Los Angeles Police Academy
Los Angeles, California
James A. Merchant, MD, DrPH
UI Injury Prevention
Research Center
Iowa City, Iowa
Sharon Ness, RN
Local 141, United Staff Nurses
Union, UFCW
Federal Way, Washington
Corinne Peek-Asa, PhD
UCLA SCIPRC
Los Angeles, California
Gwendolyn Puryear Keita, PhD
American Psychological
Association
Washington, DC
Robyn Robbins
United Food and Commercial
Workers International Union
Washington, DC
Jonathan Rosen, MS, CIH
New York State Public Employees
Federation
Latham, New York
Linda Rosenstock, MD
National Institute for
Occupational Safety and Health
Centers for Disease Control
and Prevention
Washington, DC
Eugene A. Rugala
National Center for the Analysis
of Violent Crime
Supervisory Special Agent
FBI Academy
Quantico, Virginia
Carol Runyan, PhD, MPH
UNC Injury Prevention
Research Center
Chapel Hill, North Carolina
Dan Sosin, MD, MPH
National Center for Injury
Prevention and Control
Centers for Disease Control
and Prevention
Atlanta, Georgia
Rebecca A. Speer, JD
Law Offices of Rebecca A. Speer
San Francisco, California
Larry Stoffman
Canadian Council UFCW
Vancouver, British Columbia
Jeff Thurston, MN, ARNP
Service Employees International
Union
Western State Hospital
Tacoma, Washington
Richard Titus, PhD
Office of Research and Evaluation
National Institute of Justice
Washington, DC
Barbara Webster
Liberty Mutual Research Center
for Safety and Health
Hopkinton, Maryland
Carol Wilkinson, MD, MPH
IBM Corporation
Armonk, New York
Jan Williams, CSW-R, BCD, CEAP
Corning Incorporated
Corning, New York
Craig Zwerling, MD, PhD, MPH
UI Injury Prevention
Research Center
Iowa City, Iowa
Additional copies of this report
are available from the UI IPRC,
100 Oakdale Campus, 158 IREH,
Iowa City, IA 52242-5000, or at
the IPRC web site at www.public-
health.uiowa.edu/iprc, or by
sending an e-mail to:
Editor: Leslie Loveless
Designer: Patti O’Neill
Illustrator: Luba Lukova

THE UNIVERSITY OF IOWA
R13/CCR717056-01
R49/CCR703640-11
17551/1-01
The first steps have been taken. Funding for research into what works,
and what doesn’t, is urgently needed.
AFSCME
UNION LABOR

16
THE UNIVERSITY OF IOWA
100 Oakdale Campus
158 IREH
Iowa City, IA 52242-5000
